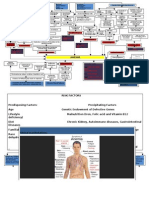
Clinical Profile Physical Findings
45 y.o Hypotensive
Male Tachycardic
Farmer, resides in Palo, Leyte Tachypneic
Sudden localized, burning, epigastric pain PRS 7/10, Afebrile
nonradiating, aggravated by food intake slightly re-
lieved by Aluminum-magnesium hydroxide
Normal oxygen saturation
Body malaise Orthopneic
Dizziness In respiratory distress
Recurrent burning, localized epigastric pain PRS 9/10, Poor capillary refill
aggravated by food intake slightly relieved by Alumi- Lips & Mucosa: Pale
num-magnesium hydroxide Gums: Pale pink
Melena Epigastric direct tenderness (+)
2019: Acute gouty arthritis Presence of tarry stool on gloves after DRE.
Fond of coffee Pivot: Melena
Ddx: Esophageal Varices Ddx: Upper GI malignancy Ddx: Acute gastritis Peptic Ulcer Disease Ddx: Schistosomiasis Ddx: Hemorrhagic & erosive
gastropathy
(Gastric vs Duodenal Ulcer)
R/I: R/I: R/I: R/I: R/I: R/I:
Melena Male Melena Farmer Possibility of NSAID abuse
Dizziness Epigastric pain Recurrent burning pain in Gastric Duodenal Endemic in Palo
epigastric area Alcoholic
Generalized pallor Melena Abdominal Pain
Symptoms of Anemia Melena
Body malaise Diarrhea Burning epigastric Burning epigastric Melena
(generalized pallor, slow pain pain Abdominal pain
Tachycardia Body weakness Tachycardic Pain precipitated
capillary refill) by food intake
Tachypnea Generalized Pallor Hypotensive R/O:
Melena Tachycardic R/O:
Low diastolic blood pressure 10 pack-year smoker Poor Hypotensive No rash
socioeconomic Melena No dyspepsia
R/O: status Poor
No itchiness No nausea
R/O: R/O: Heavy coffee socioeconomic No fever & chills
No nausea drinker status No vomiting
No hematemesis Absence of mass Smoker Heavy coffee No cough
No hematemesis Possibility of NSAID drinker No loss of appetite
No known liver disease No unintentional weight loss abuse Smoker No muscle pain
No bloated abdomen No fever
No easy bruising No early satiety Possibility of No enlarged liver
No indigestion R/O: NSAID abuse
No jaundice No Nausea & vomiting No disturbance of No hematuria
sleep d/t pain R/O:
No syncope No indigestion Pain is alleviated Cannot totally rule
No seizures
No ascites No dysphagia by food intake out No hematochezia
Admitting diagnosis: Peptic ulcer disease
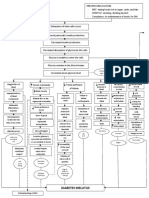
Pathophysiology
Inhibition of COX-1 in GIT
leads to reduction of
prostaglandin secretion &
cytoprotective effects in
Frequent Coffee intake Skips Meals Farmer Poor socioeconomic Status Possible abuse of NSAIDS gastric mucosa w/c in-
creases susceptibility to
mucosal injury
Irritation to gastric mucosa Acid & Pepsinogen release w/ Chronic H. pylori infection Production of urease that
vagal response to increased stress catalyzes hydrolysis of urea
to ammonia
Increased gastrin secretion
Increased gastric acid production
Weakness, body malaise
Epigastric Pain Damage/Erosion of the mucosa Inflammation
Ulcer detection:
To r/o other causes : Formation of Ulcers Barium studies of proximal GIT:
appearance of discrete ulcer wall
Liver function tests: normal craters
Amylase: normal
Lipase: normal Upper endoscopy : presence of a
Gastrointestinal bleeding Dehydration well-demarcated break in the
mucosa that may extend into the
muscularis propria of
Iron deficiency anemia
the duodenum
Melena Tachycardia Hypotensive
Note: H. pylori infection:
Hypotension Tachypnea Rapid urease test : positive
Serology (H.pylori test) : positive
CBC: Stool exam: Stool antigen: Positive
RBC: decreased
WBC: normal
Hgb: decreased No ova or parasite seen
Hct: decreased
MCHC: decreased
MCV: decreased Reduced urinary output
RDW: increased Raised creatinine
Platelet: decreased
NLMEB: normal Reduced eGFR
Increased urea:creatinine ratio
Iron studies: Electrolytes :
Serum iron: decreased NaKCl: increased
Transferrin/TIBC: increased Urinalysis:
Transferrin saturation: decreased Increased urine S.G
Ferritin: decreased
Soluble transferrin receptor: increased
You might also like
- Maxwell Quick Medical Reference PDFDocument35 pagesMaxwell Quick Medical Reference PDFAnonymous fj68Ms100% (10)
- Usmle Step 1 Study Plan by YaboiDocument10 pagesUsmle Step 1 Study Plan by Yaboimattq100% (2)
- Pathophysiology of Prostate CancerDocument3 pagesPathophysiology of Prostate Cancermkho100% (1)
- Pathoma ChecklistDocument3 pagesPathoma ChecklistDiorella Marie López GonzálezNo ratings yet
- OB 1st PNCUDocument8 pagesOB 1st PNCUAngelo Erispe100% (1)
- Concept Map Hypercalcemia Part 2Document2 pagesConcept Map Hypercalcemia Part 2Queenie Rose ArsenalNo ratings yet
- Aan 202 CourseworkDocument17 pagesAan 202 CourseworkCris GalendezNo ratings yet
- POTTs Disease PathoDocument3 pagesPOTTs Disease PathoEdgel QuidolesNo ratings yet
- Detailed 6 Week Study Schedule UsmleDocument43 pagesDetailed 6 Week Study Schedule Usmlecansemerci86% (7)
- OINA Table PDFDocument16 pagesOINA Table PDFMichelle Joy Delos Reyes100% (1)
- All Therapy 200 RATOS 2010Document284 pagesAll Therapy 200 RATOS 2010Bhargavi SunkiNo ratings yet
- Ate Mitch HN DRUG STUDYDocument23 pagesAte Mitch HN DRUG STUDYMarice VenNo ratings yet
- Im - Ugib Pud Concept MapDocument3 pagesIm - Ugib Pud Concept MapTrisNo ratings yet
- Generic Name Brand Name Drug Class Mechanism of Action StructureDocument4 pagesGeneric Name Brand Name Drug Class Mechanism of Action StructurenoelkiddoNo ratings yet
- PATHOPHYSIOLOGYDocument2 pagesPATHOPHYSIOLOGYmadelaine_espiritu0% (1)
- Anatomy and Physiology-AppendicitisDocument3 pagesAnatomy and Physiology-AppendicitisMaria Socorro Sismundo DavidNo ratings yet
- Drug StudyDocument7 pagesDrug StudyCharmz_asherahNo ratings yet
- GERD Pathophysiology Cleveland ClinicDocument17 pagesGERD Pathophysiology Cleveland ClinicMavisNo ratings yet
- Pathophysiology of Breast Cancer: If Not TreatedDocument1 pagePathophysiology of Breast Cancer: If Not TreatedsteffiNo ratings yet
- HPN Drug StudyDocument4 pagesHPN Drug StudyJohn Haider Colorado GamolNo ratings yet
- Dosage & Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing Responsibility Rivotril ClassificationDocument5 pagesDosage & Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing Responsibility Rivotril ClassificationJenyl BajadoNo ratings yet
- Pharma CompilationDocument32 pagesPharma CompilationJustin Kaye DariaNo ratings yet
- Pathophysiology of Multiple Myeloma OkDocument3 pagesPathophysiology of Multiple Myeloma OkRifa'atul MahmudahNo ratings yet
- Patho of CA & Breast CaDocument3 pagesPatho of CA & Breast CaAngeline EspinasNo ratings yet
- Cardiovascular SystemDocument26 pagesCardiovascular SystemJenny Torreda100% (1)
- Covid 19 (Case 1)Document53 pagesCovid 19 (Case 1)cendy andestriaNo ratings yet
- Dengue PathophysioDocument4 pagesDengue PathophysioHonhon MacasaquitNo ratings yet
- Pathophy - Nephrotic SyndromeedDocument1 pagePathophy - Nephrotic Syndromeedianecunar100% (1)
- Anemia Pathophysiology All in 1 by Francis OliverosDocument3 pagesAnemia Pathophysiology All in 1 by Francis Oliverosfrancis00090No ratings yet
- DRUG STUDY-danaDocument3 pagesDRUG STUDY-danairish_estrellaNo ratings yet
- Aling Juana, 42 Years Old, FemaleDocument2 pagesAling Juana, 42 Years Old, FemaleGenynne RagasaNo ratings yet
- Gastric CancerDocument7 pagesGastric CancerMicah PingawanNo ratings yet
- Assessment of Fetal Well-Being 1. Fetal MovementDocument6 pagesAssessment of Fetal Well-Being 1. Fetal MovementClaire Julianne CapatiNo ratings yet
- Pathophysiology of GooDocument2 pagesPathophysiology of GooTania Noviza100% (1)
- RevalidaDocument5 pagesRevalidaHawkins FletcherNo ratings yet
- Pathophysiology of Transitional Cell CarcinomaDocument10 pagesPathophysiology of Transitional Cell CarcinomaJheanAlphonsineT.MeansNo ratings yet
- Concept Map para ThyroidDocument7 pagesConcept Map para ThyroidAllene PaderangaNo ratings yet
- Renal MedsurgDocument14 pagesRenal MedsurgCliff Lois ╭∩╮⎷⎛⎝⎲⏝⏝⎲⎠⎷⎛╭∩╮ Ouano100% (1)
- Biliary AtresiaDocument8 pagesBiliary AtresiaBrooke MauriNo ratings yet
- Cardiogenic Shock (BSN 3b)Document7 pagesCardiogenic Shock (BSN 3b)Laurence ZernaNo ratings yet
- Pathophysiology of Hypertension, Diabetes, Ubm, BPHDocument3 pagesPathophysiology of Hypertension, Diabetes, Ubm, BPHCarly Beth Caparida LangerasNo ratings yet
- RHD PathophysiologyDocument3 pagesRHD PathophysiologyRichmond LacadenNo ratings yet
- Pathophysiology Precipitsting Factors: Predisposing FactorsDocument2 pagesPathophysiology Precipitsting Factors: Predisposing FactorsGeofrey MaglalangNo ratings yet
- CKD + HPN Concept Map DRAFTDocument1 pageCKD + HPN Concept Map DRAFTInah Floresta BesasNo ratings yet
- What Are Liver EnzymesDocument2 pagesWhat Are Liver EnzymesAAANo ratings yet
- 55-Year-Old, Male With CopdDocument3 pages55-Year-Old, Male With CopdRyrey Abraham PacamanaNo ratings yet
- Vii. Pathophysiology A. AlgorithmDocument2 pagesVii. Pathophysiology A. AlgorithmJonna Mae TurquezaNo ratings yet
- Case Scenario CsDocument6 pagesCase Scenario CsDhie Jhay InigoNo ratings yet
- DPatho ProstateDocument2 pagesDPatho Prostateshujin_sama100% (1)
- Concept MapDocument4 pagesConcept MapChelsyann FerolinoNo ratings yet
- Pathophysiology of PoisoningDocument2 pagesPathophysiology of PoisoninggoyaNo ratings yet
- SARS PathophysioDocument2 pagesSARS PathophysioLouise BravoNo ratings yet
- Cancer Chemotherapy: Acronym of RegimenDocument13 pagesCancer Chemotherapy: Acronym of RegimenVaibhav Bharat100% (1)
- Diabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)Document3 pagesDiabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)John Henry ValenciaNo ratings yet
- Mycobacterium Tuberculosis: Precipitating Factors: Predisposing FactorsDocument1 pageMycobacterium Tuberculosis: Precipitating Factors: Predisposing FactorsYoko Mae Yano100% (1)
- Medical SignsDocument16 pagesMedical SignsOluwatobi FaniyiNo ratings yet
- Pediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not DiagnosedDocument2 pagesPediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not Diagnosedrolland_arrizaNo ratings yet
- Pharma - Drugs Affecting Git MotilityDocument6 pagesPharma - Drugs Affecting Git MotilityBobet ReñaNo ratings yet
- Pathophysiology of Pressure UlcersDocument1 pagePathophysiology of Pressure UlcersSTORAGE FILENo ratings yet
- Atropine: Drug Study: NCM 106 PharmacologyDocument6 pagesAtropine: Drug Study: NCM 106 PharmacologyKevin RosalesNo ratings yet
- Cholecyctitis Nursing Concept Map DocDocument1 pageCholecyctitis Nursing Concept Map DocSteffiNo ratings yet
- Abnormal Pedia ReviewerDocument6 pagesAbnormal Pedia ReviewerMarwin OditaNo ratings yet
- Table of Genetic DisordersDocument3 pagesTable of Genetic DisordersEliNo ratings yet
- Abdominal MassDocument5 pagesAbdominal MassArthana PutraNo ratings yet
- This Study Resource Was Shared Via: HypoparathyroidismDocument1 pageThis Study Resource Was Shared Via: HypoparathyroidismDeo FactuarNo ratings yet
- MedsDocument10 pagesMedssoumya vadlamaniNo ratings yet
- Rani Ti DineDocument3 pagesRani Ti DineVimae TayaoNo ratings yet
- Sketchy, Pathoma, BNB ChecklistDocument9 pagesSketchy, Pathoma, BNB ChecklistAC BCNo ratings yet
- Obgyn PT HistoryDocument4 pagesObgyn PT HistoryDr. SheikhNo ratings yet
- Dao 2013 22Document81 pagesDao 2013 22voltageiceman89% (9)
- EMB MC NO. 2020 008 Guidelines For Site ControlDocument25 pagesEMB MC NO. 2020 008 Guidelines For Site ControlTrisNo ratings yet
- TRC As of May 31 2023Document22 pagesTRC As of May 31 2023Ace QuiranteNo ratings yet
- FDA Advisory No. 2017 016Document3 pagesFDA Advisory No. 2017 016TrisNo ratings yet
- PhysicianDocument204 pagesPhysicianTrisNo ratings yet
- Interns History TemplateDocument6 pagesInterns History TemplateTrisNo ratings yet
- AMC Candidate Account GuideDocument62 pagesAMC Candidate Account GuidezhangNo ratings yet
- Menstrual DisordersDocument35 pagesMenstrual DisordersTrisNo ratings yet
- Hazardous Waste CodesDocument5 pagesHazardous Waste CodesShiina MashiroNo ratings yet
- October 2023 PRC PLE Schedule and Reminders 2Document4 pagesOctober 2023 PRC PLE Schedule and Reminders 2TrisNo ratings yet
- Most Common PathoDocument4 pagesMost Common PathoTrisNo ratings yet
- User Registration: Emb Company Registration SystemDocument7 pagesUser Registration: Emb Company Registration SystemMICHELLE grace corpuzNo ratings yet
- Table of Contents: Bacteria: Chapter 1: Gram Positive CocciDocument13 pagesTable of Contents: Bacteria: Chapter 1: Gram Positive CocciAnthony LNo ratings yet
- Contingency Plan MMCDocument17 pagesContingency Plan MMCMaui GupitaNo ratings yet
- Transporter Application ProcessDocument21 pagesTransporter Application ProcessTrisNo ratings yet
- Evidence Based Medicine: Self-Instructional ManualDocument106 pagesEvidence Based Medicine: Self-Instructional ManualTrisNo ratings yet
- October 2023 PRC PLE Schedule and Reminders 2Document4 pagesOctober 2023 PRC PLE Schedule and Reminders 2TrisNo ratings yet
- NIP OrientationDocument144 pagesNIP OrientationPatNo ratings yet
- Trans-Out Orders: NSVD Admitting Notes Postpartum OrdersDocument7 pagesTrans-Out Orders: NSVD Admitting Notes Postpartum OrdersDre ValdezNo ratings yet
- DSM V - TocDocument9 pagesDSM V - Tocjv10gmailNo ratings yet
- Osce PediaDocument17 pagesOsce PediaJohn Christopher LucesNo ratings yet
- Clinical Case 01-2019 by SlidesgoDocument40 pagesClinical Case 01-2019 by Slidesgofind myNo ratings yet
- Basics of Pharmacoeconomics and Outcomes ResearchDocument48 pagesBasics of Pharmacoeconomics and Outcomes ResearchArvind NagNo ratings yet
- FebruariDocument985 pagesFebruaririniNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Kejadian Dispepsia Pada Pasien Di Wilayah Kerja Puskesmas Bangkinang Kota Rinda FithriyanaDocument12 pagesFaktor-Faktor Yang Berhubungan Dengan Kejadian Dispepsia Pada Pasien Di Wilayah Kerja Puskesmas Bangkinang Kota Rinda FithriyanaSofia NaimahNo ratings yet
- Na HCO3Document2 pagesNa HCO3Niño Karol Zamora100% (1)
- Meddg: A Large-Scale Medical Consultation Dataset For Building Medical Dialogue SystemDocument9 pagesMeddg: A Large-Scale Medical Consultation Dataset For Building Medical Dialogue SystemTravis BennettNo ratings yet
- Melasma e IntestinoDocument5 pagesMelasma e IntestinoRafaela MassaferaNo ratings yet
- Ebook John Murtaghs General Practice Companion Handbook PDF Full Chapter PDFDocument67 pagesEbook John Murtaghs General Practice Companion Handbook PDF Full Chapter PDFroberto.duncan209100% (26)
- Ann Hall Correction26Document3 pagesAnn Hall Correction26Dr. Emad Elbadawy د عماد البدويNo ratings yet
- Chemistry ProjectDocument14 pagesChemistry ProjectDebabrata NagNo ratings yet
- KushtaDocument3 pagesKushtaDrMohamed RifasNo ratings yet
- What Are Symptoms of A Heart AttackDocument3 pagesWhat Are Symptoms of A Heart AttackBillieTanNo ratings yet
- Drug StudyDocument5 pagesDrug Studypaulkris_14100% (1)
- Mono Amla Phyllanthus Emblica EnglishDocument7 pagesMono Amla Phyllanthus Emblica EnglishHarshaNo ratings yet
- Gastritis 103Document16 pagesGastritis 103John Richard LuceroNo ratings yet
- Revised Drug IndexDocument76 pagesRevised Drug IndexMinette SantosNo ratings yet
- Giloy BenefitsDocument1 pageGiloy BenefitsGorav Bhalla0% (1)
- Article1381927535 - Wagh Et AlDocument14 pagesArticle1381927535 - Wagh Et AlPawan KumarNo ratings yet
- Case Study HanieeeeeeDocument40 pagesCase Study HanieeeeeeAfiq Mubasyyir Amran100% (2)
- Emergency Acupressure TreatmentDocument39 pagesEmergency Acupressure TreatmentNarayana Mugalur100% (1)
- 28 Biochemic Combination TabletsDocument6 pages28 Biochemic Combination Tabletsvprakash7972No ratings yet
- CalamineDocument4 pagesCalamineFaye FelicesNo ratings yet
- Home Remedies For Top 15 Daily Health Problems PDFDocument11 pagesHome Remedies For Top 15 Daily Health Problems PDFEmil VictorovNo ratings yet
- Peptic Ulcer Disease: by Aniedu, UgochukwuDocument32 pagesPeptic Ulcer Disease: by Aniedu, UgochukwuManish Sapkota100% (1)
- 1 - Sued in Federal Court Other Nine Crato Criminal of USADocument25 pages1 - Sued in Federal Court Other Nine Crato Criminal of USALuis Alberto Pita SantosNo ratings yet
- Gastro MCQsDocument14 pagesGastro MCQsvaegmundigNo ratings yet
- Chapter 13 Heartburn and DyspepsiaDocument10 pagesChapter 13 Heartburn and DyspepsiaPia Angelica DizonNo ratings yet
- Cynara Scolymus ArtichokeDocument8 pagesCynara Scolymus Artichokeplanet_renNo ratings yet
- Helicobacter Pylori (H. Pylori) Infection FactsDocument38 pagesHelicobacter Pylori (H. Pylori) Infection FactsPieter SteenkampNo ratings yet