You might also like
- Vibrio, Campylobacter, and HelicobacterDocument7 pagesVibrio, Campylobacter, and HelicobacterRach ReyesNo ratings yet
- Bacteriology NotesDocument10 pagesBacteriology NotesAndrei Tumarong AngoluanNo ratings yet
- Microbiology - Overview Reports and IntepretationDocument9 pagesMicrobiology - Overview Reports and IntepretationRo RyNo ratings yet
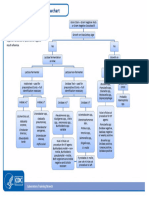
- Bacterial ID FlowchartDocument6 pagesBacterial ID FlowchartTom Tsou50% (2)
- Micro Bacteriology PDFDocument4 pagesMicro Bacteriology PDFMasroor ShahNo ratings yet
- Detailed Micro ChartDocument6 pagesDetailed Micro Chartmatt100% (1)
- MTAP - 1.1 - BacteriologyDocument14 pagesMTAP - 1.1 - BacteriologyKassandra CordetaNo ratings yet
- EPI BangladeshDocument4 pagesEPI BangladeshToufiq Rahman100% (1)
- Biochemical Tests For Staph-Strep - OutputDocument5 pagesBiochemical Tests For Staph-Strep - OutputJoshua Ty CayetanoNo ratings yet
- 3.6.8 SOP - Stool CultureDocument5 pages3.6.8 SOP - Stool CultureSemeeeJuniorNo ratings yet
- Plasmapheresis For AutoimmunityDocument14 pagesPlasmapheresis For AutoimmunityEliDavidNo ratings yet
- Spondylo ArthropathyDocument89 pagesSpondylo ArthropathyJen NeeNo ratings yet
- SMLE 13 - MedicalDocument850 pagesSMLE 13 - MedicalSumayyia QamarNo ratings yet
- Aerobic Gram Negative Rods Flowchart 508Document1 pageAerobic Gram Negative Rods Flowchart 508Issa AlejoNo ratings yet
- Hematopatologie 2016Document45 pagesHematopatologie 2016CristiNo ratings yet
- (Microbio) Staphyloccocus and Streptococcus-Dr. Salandanan (BHND)Document16 pages(Microbio) Staphyloccocus and Streptococcus-Dr. Salandanan (BHND)Lee Delos Santos100% (1)
- 8A Nosocomial InfectionDocument15 pages8A Nosocomial InfectionSuminaShrestha100% (1)
- Bacteriology Lecture MidtermsDocument13 pagesBacteriology Lecture MidtermsEvanka BaguistanNo ratings yet
- The Pathogenic Basis of Malaria: InsightDocument7 pagesThe Pathogenic Basis of Malaria: InsightRaena SepryanaNo ratings yet
- Gram Positive CocciDocument6 pagesGram Positive Coccitamiqua1No ratings yet
- Micrococcaceae and Streptococcaceae TransesDocument9 pagesMicrococcaceae and Streptococcaceae TransesaguirreangNo ratings yet
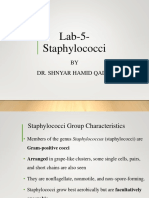
- Lab-5-Staphylococci: BY Dr. Shnyar Hamid QadirDocument24 pagesLab-5-Staphylococci: BY Dr. Shnyar Hamid QadirHanaNo ratings yet
- Differentiation of Staphylococcus From Micrococcus: Catalase Test Aerobic GrowthDocument13 pagesDifferentiation of Staphylococcus From Micrococcus: Catalase Test Aerobic GrowthPau SorianoNo ratings yet
- Laboratory 10 Identification of Streptococcus and Enterococcus SpeciesDocument3 pagesLaboratory 10 Identification of Streptococcus and Enterococcus SpeciesRazmine RicardoNo ratings yet
- Penjelasan Praktikum KardiovaskulerDocument54 pagesPenjelasan Praktikum KardiovaskulerQuswah MaharaniNo ratings yet
- Praktikum MikrobiologiDocument54 pagesPraktikum MikrobiologilarasatiNo ratings yet
- Enjelasan Praktikum Mikrobiologi Blok KardiovaskulerDocument56 pagesEnjelasan Praktikum Mikrobiologi Blok KardiovaskulerAtik LestariNo ratings yet
- W9 Bacte LAB Identification of StaphylococcusDocument27 pagesW9 Bacte LAB Identification of StaphylococcusAnne CabreraNo ratings yet
- Salmonella Serotyping: Practical ApproachDocument9 pagesSalmonella Serotyping: Practical Approachtalal101No ratings yet
- PL850 Rabbit-Coagulase-Plasma EnglishDocument2 pagesPL850 Rabbit-Coagulase-Plasma Englishzahramaulidi28No ratings yet
- Bacte Midterm (Walang Pictures)Document21 pagesBacte Midterm (Walang Pictures)AL-HUSSEIN NAWABNo ratings yet
- Aerobic Gram Negative Rods FlowchartDocument1 pageAerobic Gram Negative Rods FlowchartKeithNo ratings yet
- Gram Positive CocciDocument27 pagesGram Positive Coccishekhar JhaNo ratings yet
- Microbiology Overview: Interpretation of Preliminary Microbiology DataDocument10 pagesMicrobiology Overview: Interpretation of Preliminary Microbiology DataGustavo PieroniNo ratings yet
- Coagulase PlasmaDocument2 pagesCoagulase PlasmaHà Anh Minh LêNo ratings yet
- MicroTech Lec Reviewer FinalsDocument18 pagesMicroTech Lec Reviewer FinalsAzh Haezen Marithe TarlacNo ratings yet
- MDL 237 StaphylococciDocument66 pagesMDL 237 StaphylococcibearXDNo ratings yet
- Bacte FinalsDocument11 pagesBacte FinalsRose Denisse EstrellaNo ratings yet
- PDF Document 2Document313 pagesPDF Document 2nasarcedaNo ratings yet
- VMCB 55 Veterinary Microbiology and Bacteriology: I. AbstractDocument15 pagesVMCB 55 Veterinary Microbiology and Bacteriology: I. AbstractNuel EsguerraNo ratings yet
- Micro PrefinalDocument5 pagesMicro PrefinalfarahjundanNo ratings yet
- Pro-Lab: DiagnosticsDocument2 pagesPro-Lab: Diagnosticsapi-3742158No ratings yet
- EnterobacteriaceaeDocument8 pagesEnterobacteriaceaeWansun MaglangitNo ratings yet
- Bacteriolgy Catalase (+), Gram (+) Cocci Part 1Document4 pagesBacteriolgy Catalase (+), Gram (+) Cocci Part 1Shaniah xxNo ratings yet
- Identification of Unknown1 BacteriaDocument6 pagesIdentification of Unknown1 BacteriaAbdul WahabNo ratings yet
- Laboratory 11 EnterobacteriaceaeDocument9 pagesLaboratory 11 EnterobacteriaceaeRazmine RicardoNo ratings yet
- Practical Medical Microbiology PHT382Document22 pagesPractical Medical Microbiology PHT382mdsajidaaliNo ratings yet
- Labmed32 0368Document8 pagesLabmed32 0368shennie anteNo ratings yet
- Lab 6Document5 pagesLab 6moodyNo ratings yet
- 2019 - Identifikasi StaphylococcusDocument18 pages2019 - Identifikasi StaphylococcusDanny. JayNo ratings yet
- Student Notes: Micro 1: Davao Doctors College Medical Laboratory Science DepartmentDocument5 pagesStudent Notes: Micro 1: Davao Doctors College Medical Laboratory Science DepartmentMelody Jane PardilloNo ratings yet
- Pratical Two ReportDocument13 pagesPratical Two ReportMUBIRU SAMUEL EDWARDNo ratings yet
- Student Notes: Micro 1: Davao Doctors College Medical Laboratory Science DepartmentDocument2 pagesStudent Notes: Micro 1: Davao Doctors College Medical Laboratory Science DepartmentMelody Jane PardilloNo ratings yet
- Simple Guide Identification Bacteria: Dr. Khalil AlkuwaityDocument18 pagesSimple Guide Identification Bacteria: Dr. Khalil AlkuwaitySaid IsaqNo ratings yet
- Week 8 - Bacteriology LectureDocument7 pagesWeek 8 - Bacteriology LectureReangg SerranoNo ratings yet
- Bacte Midterm Di TaposDocument9 pagesBacte Midterm Di TaposAL-HUSSEIN NAWABNo ratings yet
- Non-Fermenting & Miscellaneous Gram-Negative BacilliDocument12 pagesNon-Fermenting & Miscellaneous Gram-Negative Bacillisvurbina3934valNo ratings yet
- Practical Session Two Guide-1Document9 pagesPractical Session Two Guide-1Andrease WandazNo ratings yet
- MB - Day 2Document9 pagesMB - Day 2online medtekNo ratings yet
- Mannitol Salt AgarDocument1 pageMannitol Salt AgarJoelle DwekNo ratings yet
- Staphylococcus: Made By: Shalini BishtDocument70 pagesStaphylococcus: Made By: Shalini BishtEduardo SalazarNo ratings yet
- Staphylococcus: Made By: Shalini BishtDocument70 pagesStaphylococcus: Made By: Shalini BishtEduardo SalazarNo ratings yet
- 3 - Gram Positive BacteriaDocument7 pages3 - Gram Positive BacteriaPHAMAE JOY MEMBREVENo ratings yet
- Gram Stain For Non-MicrobiologistDocument8 pagesGram Stain For Non-MicrobiologistJoanne Faith ManayagNo ratings yet
- S Aureus (Autosaved)Document16 pagesS Aureus (Autosaved)Pitua IvaanNo ratings yet
- Lec - Bacte - Non Fermentative Gram Negative Bacilli - MidtermsDocument2 pagesLec - Bacte - Non Fermentative Gram Negative Bacilli - MidtermsJashmine May TadinaNo ratings yet
- Marion CompressedDocument112 pagesMarion CompressedPaper Application TeamNo ratings yet
- Aa by AbdifatahDocument57 pagesAa by AbdifatahAbdifatah AhmedNo ratings yet
- Acute Tonsillopharyngitis: Group BDocument52 pagesAcute Tonsillopharyngitis: Group BVivekanandaNo ratings yet
- Jurnal Alang-AlangDocument10 pagesJurnal Alang-AlangFransLei Vadoel SaelNo ratings yet
- Week 2 - Part 1 - Introduction and History of ImmunologyDocument20 pagesWeek 2 - Part 1 - Introduction and History of ImmunologySara-hJane GuintoNo ratings yet
- Comparison of The Minimum Fungicidal Concentration of Clotrimazole, Ketoconazole, Miconazole and Terbinafine Against Clinical Isolates of DermatophytesDocument4 pagesComparison of The Minimum Fungicidal Concentration of Clotrimazole, Ketoconazole, Miconazole and Terbinafine Against Clinical Isolates of DermatophytesPratik PawarNo ratings yet
- Overview of Global HIVDocument27 pagesOverview of Global HIVAhmed AdemNo ratings yet
- Immunohematology ASCPi Review Booklet (Part 1)Document22 pagesImmunohematology ASCPi Review Booklet (Part 1)Mark Justin OcampoNo ratings yet
- Pneumocystis Jirovecii Pneumonia: A Review of CurrentDocument14 pagesPneumocystis Jirovecii Pneumonia: A Review of CurrentMa No LoNo ratings yet
- Daftar Pustaka Aps OrangDocument3 pagesDaftar Pustaka Aps OrangAlexander DickyNo ratings yet
- Git, Liver & GB: by Dr. Thameem SaifDocument119 pagesGit, Liver & GB: by Dr. Thameem SaifGirija VirkarNo ratings yet
- German Gov't Bombshell - Alarming Number of Vaccinated Are Developing AIDS' - News PunchDocument8 pagesGerman Gov't Bombshell - Alarming Number of Vaccinated Are Developing AIDS' - News PunchKarla VegaNo ratings yet
- CDC Emails On Changing DefinitionsDocument67 pagesCDC Emails On Changing DefinitionsEpoch TranslatorNo ratings yet
- HIV 1 2 Ab Rapid Test Cassette 1Document5 pagesHIV 1 2 Ab Rapid Test Cassette 1Dewi LengkanawatiNo ratings yet
- Positive and Negative Filipino ValuesDocument2 pagesPositive and Negative Filipino ValuesBrenty TablateNo ratings yet
- Infection Control StudentDocument27 pagesInfection Control StudentTami CarterNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaAlmira PutriNo ratings yet
- Mast Cell Chymase Protects Against Acute Ischemic Kidney Injury by Limiting Neutrophil Hyperactivation and RecruitmentDocument40 pagesMast Cell Chymase Protects Against Acute Ischemic Kidney Injury by Limiting Neutrophil Hyperactivation and RecruitmentOmar Arias AndradeNo ratings yet
- Salmonella IgM ELISA Package InsertDocument2 pagesSalmonella IgM ELISA Package InsertHarnadi WonogiriNo ratings yet
- Dengue 2 AlertDocument4 pagesDengue 2 AlertJayant Jain100% (1)
- 03 Pemicu 4 Imun 21Document49 pages03 Pemicu 4 Imun 21vario BernardyNo ratings yet
- Kemenkes RSCM 2022 - Evaluasi Kualitatif Penggunaan Antimikroba - Fitria Nur HidayahDocument26 pagesKemenkes RSCM 2022 - Evaluasi Kualitatif Penggunaan Antimikroba - Fitria Nur HidayahrizkiameliahexshaNo ratings yet
- CH 57 Care of Patients With Inflammatory Intestinal DisordersDocument19 pagesCH 57 Care of Patients With Inflammatory Intestinal Disordersjrflores1284No ratings yet