You might also like
- My Personal SWOT Analysis For The Human Resource ManagerDocument1 pageMy Personal SWOT Analysis For The Human Resource Managerzahur27100% (2)
- Nike Case Study SolutionDocument6 pagesNike Case Study SolutionSling Shot83% (6)
- A Contingency View of Porter's "Generic Strategies"Document12 pagesA Contingency View of Porter's "Generic Strategies"Onos Bunny BenjaminNo ratings yet
- Motivational EssayDocument1 pageMotivational EssayAnne VanessaNo ratings yet
- Relay Characteristic AngleDocument14 pagesRelay Characteristic AngleAji Istanto Rambono100% (1)
- Reactance Influence On 6-Phase Rectifiers: R.L. Witzke V. KresserDocument1 pageReactance Influence On 6-Phase Rectifiers: R.L. Witzke V. KresserZulfiqar AliNo ratings yet
- Topic 3 - Measurement of Angles and DirectionsDocument3 pagesTopic 3 - Measurement of Angles and DirectionsJames Daryl TecsonNo ratings yet
- ELTK1200 Formula Sheet: Induced Voltage Power FactorDocument8 pagesELTK1200 Formula Sheet: Induced Voltage Power FactorEdson GomesNo ratings yet
- PN Junction DiodeDocument4 pagesPN Junction DiodeRajesh PylaNo ratings yet
- A Self-Directed Learning Module: Queen's University Department of Emergency MedicineDocument38 pagesA Self-Directed Learning Module: Queen's University Department of Emergency MedicinerinoNo ratings yet
- Testing Directional Overcurrent ProtectionDocument2 pagesTesting Directional Overcurrent ProtectionZokiNo ratings yet
- Chapter 3 Compass SurveyingDocument39 pagesChapter 3 Compass Surveyingdusamouscrib2014No ratings yet
- Basic Laws 2Document21 pagesBasic Laws 2Bendera Hitam Dari TimurNo ratings yet
- 1.6.3 Mutually Related Reference Polarity of Current/voltageDocument1 page1.6.3 Mutually Related Reference Polarity of Current/voltageanothersomeguyNo ratings yet
- EE202-S24 w02 1 Sinusoids-And-PhasorsDocument22 pagesEE202-S24 w02 1 Sinusoids-And-Phasorsogkrdmn58No ratings yet
- Experiment 05Document3 pagesExperiment 05himanshu yadavNo ratings yet
- MagntismDocument23 pagesMagntismUsman qadriNo ratings yet
- Angles and Directions SurveyingDocument23 pagesAngles and Directions SurveyingAbel AmmoNo ratings yet
- Bsaic of RsistorsDocument33 pagesBsaic of Rsistorsmohamed shabbanNo ratings yet
- Notes by Guy Fletcher VK2KU: Complex Impedance MeterDocument3 pagesNotes by Guy Fletcher VK2KU: Complex Impedance MeterR.Dimas DityagrahaNo ratings yet
- Electrostatics (Formula Sheet)Document6 pagesElectrostatics (Formula Sheet)Sukanya PaulNo ratings yet
- Chapter 6Document26 pagesChapter 6Mohammad SaabNo ratings yet
- KVL PDFDocument2 pagesKVL PDFMohammad Suhail KhanNo ratings yet
- 4-Magnetic Effect 2021Document27 pages4-Magnetic Effect 2021Shamit MNo ratings yet
- Network Anal 2020Document17 pagesNetwork Anal 2020chuariwapoohNo ratings yet
- Tutorial 1bDocument2 pagesTutorial 1bmiindsurferNo ratings yet
- Electrical Axis and Axis Deviation: Fig. 6.1CDocument9 pagesElectrical Axis and Axis Deviation: Fig. 6.1CFelipe GallardoNo ratings yet
- Mechanics of Materials NtesDocument59 pagesMechanics of Materials NtesP R VenkateshNo ratings yet
- 11-Fault Locator With 2 Ended MeasurementDocument14 pages11-Fault Locator With 2 Ended MeasurementtajudeenNo ratings yet
- Chapter 10Document9 pagesChapter 10kdalavadi3905No ratings yet
- G. Measurement of Angles and DirectionsDocument3 pagesG. Measurement of Angles and DirectionsJasleneDimarananNo ratings yet
- Emi Exp 3Document4 pagesEmi Exp 3Virag ParekhNo ratings yet
- Lab 01: Orientation of Lines & Planes in Rocks: Collaborators Using Precise Terminology and SymbolsDocument5 pagesLab 01: Orientation of Lines & Planes in Rocks: Collaborators Using Precise Terminology and SymbolsLUIS FERNANDO QUISPE QUISPENo ratings yet
- Study of DiodeDocument3 pagesStudy of DiodeSai pavanNo ratings yet
- Electrical Axis and Axis Deviation: Mean Qrs Axis: DefinitionDocument9 pagesElectrical Axis and Axis Deviation: Mean Qrs Axis: Definitionrocker_jadulNo ratings yet
- Group 1 KheimDocument4 pagesGroup 1 KheimWriznym SampangNo ratings yet
- BEE Unit3Document50 pagesBEE Unit3Aman PailwanNo ratings yet
- 11 Chapter3Document46 pages11 Chapter3Anonymous wAdxNydjNo ratings yet
- Circular MotionDocument13 pagesCircular MotionShakeel AhmadNo ratings yet
- Physics Practicals VIIDocument33 pagesPhysics Practicals VIIJerin K MNo ratings yet
- Electrical Engineering (p149-175)Document27 pagesElectrical Engineering (p149-175)Josh DejascoNo ratings yet
- Network Laws & TheoremsDocument14 pagesNetwork Laws & Theoremstroy guillNo ratings yet
- Kirchoff's Voltage Law: V + V + V - 10 0 Resulting KVL EquationDocument2 pagesKirchoff's Voltage Law: V + V + V - 10 0 Resulting KVL EquationnichkhunieNo ratings yet
- 2103-Abj - Note - Fluid Mechancis - Conventions For The Angles Beta and Alpha For Turbomachine Blades and Euler and Mechanical Power PDFDocument6 pages2103-Abj - Note - Fluid Mechancis - Conventions For The Angles Beta and Alpha For Turbomachine Blades and Euler and Mechanical Power PDFMǾhămed TăwfiķNo ratings yet
- Day 3 03 Directional OvercurrentDocument19 pagesDay 3 03 Directional OvercurrentVHMANOHARNo ratings yet
- Lec 16Document17 pagesLec 16Subhadeep PaladhiNo ratings yet
- Unit 4 Module 1 Lecture 2Document25 pagesUnit 4 Module 1 Lecture 2anmolbansal1969No ratings yet
- Zener DiodeDocument6 pagesZener DiodeRajesh PylaNo ratings yet
- 4.magnetic Effects of Current and MagnetismDocument133 pages4.magnetic Effects of Current and MagnetismRishit JainNo ratings yet
- Compass SurveyingDocument37 pagesCompass SurveyingGame LoverNo ratings yet
- Example 23.10: An Infinite Line Charge or Charged Conducting CylinderDocument2 pagesExample 23.10: An Infinite Line Charge or Charged Conducting CylinderOscar JavierNo ratings yet
- L2 Electrostatics Update1 SIDocument34 pagesL2 Electrostatics Update1 SIjihadNo ratings yet
- Lab 4 Linear Polarization (April 2006)Document10 pagesLab 4 Linear Polarization (April 2006)Anonymous QrHxJ4No ratings yet
- Chapter - 18 Current ElectricityDocument48 pagesChapter - 18 Current Electricityashiq3pNo ratings yet
- Lecture 04Document79 pagesLecture 04Adeel ZafarNo ratings yet
- Experiment 03Document5 pagesExperiment 03himanshu yadavNo ratings yet
- Waveform Generators and Nonlinear Circuits: 3.1 Zero-Crossing DetectorsDocument15 pagesWaveform Generators and Nonlinear Circuits: 3.1 Zero-Crossing DetectorsAndrewNo ratings yet
- Chapter 23 Electric PotentialDocument12 pagesChapter 23 Electric PotentialDinanti PratiwiNo ratings yet
- Experiments After BTDocument11 pagesExperiments After BTArkaprava MukherjeeNo ratings yet
- Basic 2 Workbook Unit 6Document6 pagesBasic 2 Workbook Unit 6Libnim GarciaNo ratings yet
- PDPR Bahasa Inggeris Tahun 5 12 July 2021 / MondayDocument12 pagesPDPR Bahasa Inggeris Tahun 5 12 July 2021 / MondayKiran KaurNo ratings yet
- Fingerprint Prediction Enabled Passport Authentication SystemDocument3 pagesFingerprint Prediction Enabled Passport Authentication SystemBalaji TriplantNo ratings yet
- Geometrical Properties Material Properties: Design of Saw Tooth/Slabless StairDocument4 pagesGeometrical Properties Material Properties: Design of Saw Tooth/Slabless Stairfoush bashaNo ratings yet
- Bengaluru's Guidance Value To Go Up by 30 - 100% - Citizen Matters, BengaluruDocument3 pagesBengaluru's Guidance Value To Go Up by 30 - 100% - Citizen Matters, BengalururtkaushikNo ratings yet
- Excavator O&KDocument8 pagesExcavator O&Keknasius iwan sugoro100% (2)
- Dynamic Performance Analysis of Permanent Magnet Hybrid Stepper Motor by Transfer Function Model For Different Design TopologiesDocument7 pagesDynamic Performance Analysis of Permanent Magnet Hybrid Stepper Motor by Transfer Function Model For Different Design TopologiesEEEENo ratings yet
- Mini Flow Channel ExperimentDocument9 pagesMini Flow Channel Experimentpotato92No ratings yet
- Top HTML and HTML5 Interview Questions (2021) - InterviewBitDocument59 pagesTop HTML and HTML5 Interview Questions (2021) - InterviewBitGaurav GhoshNo ratings yet
- Syllabus - Momentum Transfer Lec and LabDocument6 pagesSyllabus - Momentum Transfer Lec and LabKzenetteNo ratings yet
- Procedure For Carrying Out Amendments: Sl. No. Revision NO. NO. Summary of Amendments Date Drawn CheckedDocument1 pageProcedure For Carrying Out Amendments: Sl. No. Revision NO. NO. Summary of Amendments Date Drawn CheckedkarthikNo ratings yet
- How To Use Radiofacsimile Weather MapsDocument29 pagesHow To Use Radiofacsimile Weather MapsJerry HigdonNo ratings yet
- Normed Vector SpaceDocument5 pagesNormed Vector Spacesreekantha2013No ratings yet
- Presentation of Godrej CompanyDocument15 pagesPresentation of Godrej CompanyRiya TopiwalaNo ratings yet
- Personal Loan AgreementDocument2 pagesPersonal Loan AgreementFebb RoseNo ratings yet
- AssignmentDocument6 pagesAssignmentAkshay MehtaNo ratings yet
- Leo Lastimosa ProfileDocument3 pagesLeo Lastimosa ProfileTrey JakosalemNo ratings yet
- "ABP Postgraduate Diploma in Business Management": Assignment: Management of Financial Resources and PerformanceDocument3 pages"ABP Postgraduate Diploma in Business Management": Assignment: Management of Financial Resources and PerformancenilangaxNo ratings yet
- Mucoadhesive DDS - 1749098145Document14 pagesMucoadhesive DDS - 1749098145Vaibhav ThoratNo ratings yet
- HCG Diet Personal Tracking GuideDocument6 pagesHCG Diet Personal Tracking GuideGregorio ReyNo ratings yet
- Lecture 13 - Lumber GradingDocument20 pagesLecture 13 - Lumber GradingimanolkioNo ratings yet
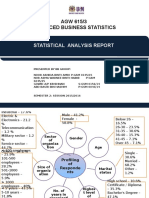
- AGW 615/3 Advanced Business Statistics: Statistical Analysis ReportDocument10 pagesAGW 615/3 Advanced Business Statistics: Statistical Analysis ReportNida AmriNo ratings yet
- 105 Mid-Week AssignmentDocument4 pages105 Mid-Week AssignmentSandhya SharmaNo ratings yet
- Healthmedicinet I 2017 2Document598 pagesHealthmedicinet I 2017 2tuni santeNo ratings yet
- CJHP 66 369Document6 pagesCJHP 66 369lia pramudha wardhaniNo ratings yet
- Enc28j60 HDocument12 pagesEnc28j60 HMokhammad Sanpradipto JaluntoroNo ratings yet