Professional Documents
Culture Documents
Inecquality
Uploaded by
pratamayossi41Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Inecquality
Uploaded by
pratamayossi41Copyright:
Available Formats
A systematic review of the effectiveness of
health service interventions aimed at reducing
inequalities in health
Lorna Arblaster. Mark Lambert*. Vikki Entwistle t • Martin Forster;. Deirdre Fullerton t •
Trevor Sheldon t • Ian Watt t
*United Health Commission, South Humberside; tNHS Centre for Reviews and Dissemination, University of York; ~Department of Economics
and Related Studies, University of York, UK
Objective: To review the available evidence in order to identify effective interventions which health services alone or
in collaboration with other agencies could use to reduce inequalities in health.
Methods: A search of the literature was undertaken using a number of databases including Medline (from 1990),
Applied Social Science Index and Abstracts (1987-1994), and the System for Information on Grey Literature in
Europe (1984-1994), on a large range of key words. Studies were included if they assessed interventions designed to
reduce inequalities in health or improve the health of a population group relevant to the review, and could be carried
out by a health service alone or in collaboration with other agencies. Only studies evaluating interventions using an
experimental design were included. Papers in any language were considered. In addition, systematic reviews of the
research on the effectiveness of health promotion and the treatment of conditions where there are significant health
inequalities were identified in order to illustrate the potential for reducing inequalities in health.
Results: 94 studies were identified which satisfied all the inclusion criteria and 21 reviews were included. A number
of interventions have been shown to improve the health of groups who are disadvantaged by socio-economic class,
ethnicity or age and, if properly targeted, could be expected to reduce health inequalities. H a health intervention
is being used, there should be evidence that it has an impact on health status. Attention should then be given to the
way in which the intervention is delivered and the characteristics of a programme to promote implementation.
Characteristics of successful interventions specifically aimed at reducing health differentials include: systematic
and intensive approaches to delivering effective health care; improvement in access and prompts to encourage
the use of services; strategies employing a combination of interventions and those involving a multi-disciplinary
approach; ensuring interventions address the expressed or identified needs of the target population; and the involve-
ment of peers in the delivery of interventions. However, these characteristics alone are not sufficient for success, nor
are they universally necessary.
Conclusions: Although it is likely that the most significant contributions to reducing health inequalities will be
in improving economic and social conditions and the physical environment, there are interventions which health
services, either alone or in collaboration with other agencies, can use to reduce inequalities in health.
Journal of Health Services Research and Policy Vol. 1 No 2,1996: 93-103 © Pearson Professional Ltd 1996
Introduction Concern about the implications of these inequalities
has led to the commissioning of a number of govern-
Levels of health in Western countries have steadily im-
ment reports." As part of the government's report for
proved during this century. Despite this, inequalities in
England.! the NHS Centre for Reviews and Dissemina-
health have persisted throughout the post Second World
tion (CRD) carried out a systematic review of evaluations
War era and, in recent years, inequalities in mortality
of interventions aimed at increasing the poor health of
rates between socio-economic groups in some countries
disadvantaged groups.' This paper reports the results of
have been increasing.'
an extended review with the aim of identifying health
care interventions which health services can use alone or
Lorna Arblaster MBBS, Independent Researcher, Mark Lambert
MBBS, Senior Registrar in Public Health Medicine, United Health in collaboration with other agencies to reduce inequali-
Commission, South Humberside; Vikki Entwistle PhD, Research ties in health. The health categories considered are: acci-
Fellow; Deirdre Fullerton MSc, Research Fellow; Trevor Sheldon MSc, dents; cancers; coronary heart disease (CHD)jstroke;
Professor; Ian Watt MPH, Honorary Consultant in Public Health
Medicine, NHS Centre for Reviews and Dissemination, University of sexual health and mental illness (areas prioritized as part
York, York YOI 5DD, UK Martin Forster MSc, Postgraduate Student, of the government's strategy for health in England") as
Department of Economics and Related Studies, University of York, well as pregnancy and childbirth. The main inequalities
York, UK Correspondence to TS.
considered are those related to socio-economic status,
J Health Serv Res Policy Volume 1 Number 2 April 1996 93
A systematic review of the effectiveness of health service interventions Review article
age and ethnicity. Consideration of other areas such as interventions aimed at reducing health inequalities were
oral health, child health and development and nutrition reviewed.
are the subject of a further extension to this review. These papers were identified via a search of the litera-
The factors which influence inequalities in health have ture using a number of computerized databases includ-
been described extensively.l" Benzeval and colleagues? ing Medline (from 1990), Applied Social Science Index
have proposed a framework for tackling them which sug- and Abstracts (1987-1994), and the System for Informa-
gests four levels for intervention: improving the physical tion on Grey Literature in Europe (1984-1994), on a
environment; addressing social and economic factors; large range of key words. In addition two existing reviews
reducing barriers to adopting a healthier personal life- relevant to this area,B,g experts, people attending relevant
style; and improving access to appropriate and effective conferences and a UK network of public health practi-
health and social services. tioners were used to identify studies. More details are
In focusing only on interventions which health serv- provided elsewhere."
ices either alone or in collaboration with other agencies The papers were checked for relevance according to
can use to address health inequalities, this paper ignores health outcomes and the target population. Studies were
many of the options contained within Benzeval's frame- included if they assessed interventions designed to re-
work. No consideration is given here to addressing the duce inequalities in health or to improve the health of a
more fundamental inequalities which exist in society and population group in the health areas detailed in the in-
which are linked to inequalities in health. troduction, and could be carried out by health services
The interventions considered in this paper fall into alone or in collaboration with other agencies. Studies
two main categories: had to report outcomes which were either health out-
comes or intermediate outcomes for which the reviewers
1. Those which target effective health services or inter-
were aware of evidence of an impact on health (e.g.
ventions at the groups with the greatest health needs.
smoking), or it was plausible that there was an impact on
For example, there exist marked social class inequali-
health. Only intervention studies with an experimental
ties in the rate of childhood accidents. Therefore, an
design (before after studies with or without controls;
intervention designed to reduce these accidents, if
randomized and non-randomized) were included. Pa-
equally effective in all social classes (or more effective
pers in any language were considered, though only those
in disadvantaged groups), could reduce social class
studies relevant to developed countries were included.
inequalities.
Since intervention settings, populations and health out-
2. Specific interventions to reduce morbidity in age, sex,
comes were extremely diverse, a narrative review of the
socio-economic and ethnic groups suffering poorer
individual study results was carried out in an attempt to
health outcomes (e.g. specific uptake promotion ac-
identify relevant characteristics.
tivities targeted at women in disadvantaged groups
who have an abnormal cervical smear result) .
Literature addressing the first of these strategies is not Summary of reviews assessing the
considered in a comprehensive way since it would mean effectiveness of health care interventions
a review of the effectiveness of all health care interven-
tions in which relevant groups had poorer health out- This section summarizes the results of reviews which
comes. However, by summarizing a number of reviews in assess the success health care interventions have had in
specific health areas, it is possible to illustrate how the influencing specific health outcomes or their associated
results of such reviews can be applied to health inequali- risk factors, arranged by health category. For each health
ties. This paper also summarizes the results of nearly category, a brief discussion of the inequalities addressed
100 evaluations of specific interventions to improve in this paper is presented before the relevant reviews
health in disadvantaged groups which fall into the are summarized and, where necessary, reference is
second category detailed above. made to interventions which have demonstrated success
at improving the health outcome of a disadvantaged
group.
Methods
In order to assess evaluations of interventions aimed
Accidents
at reducing inequalities in specific health categories, 21
relevant systematic reviews were identified using a series In the UK, unintentional injury in childhood is the lead-
of reviews of health promotion commissioned by the ing cause of death in those aged 1-15 years and deaths
NHS Centre for Reviews and Dissemination and related from unintentional injury have a steeper occupational
databases. Results of these reviews are presented by social class gradient than any other cause of death in
health category in the next section and, where possible, childhood." Older people are also at high risk of acci-
are supplemented by examples of specific interventions dents with more than eight times as many people over 65
which have demonstrated success at improving the health as under 15 dying annually as a result of accidents in the
of a disadvantaged group. UK..II The targeting of effective interventions at children
To identify characteristics that could affect the success in more deprived communities and at older people may
of such interventions, 94 papers reporting evaluations of reduce some of these inequalities.
94 J Health Serv Res Policy Volume 1 Number 2 April 1996
Review article A systematic review of the effectiveness of health service interventions
1. Accident prevention in children and adolescents stop and informing smokers that their progress will be
checked on subsequent visits.
Towner et al" reviewed 135 studies and 9 reviews eva-
Sanders" found that the more intensive the interven-
luating interventions aimed at tackling unintentional
tion, the higher the likely success rate. Simple techniques
injuries on the road, in the home and in the leisure envi-
such as putting reminder stickers on a patient's notes
ronment. The interventions shown to be most successful
increased the effectiveness of advice, and when staff were
at reducing childhood injury include promotion of bicy-
given additional training in methods of helping smokers
cle helmet use by legislation or education; promoting
to quit, their motivation to discuss smoking increased.
the use of child restraint devices and seat belts using le-
Sanders" recommends that primary care facilitators and
gislation, education and loan schemes; area-wide urban
health promotion departments should provide relevant
safety measures such as traffic calming; and educating
short, accessible training programmes with follow-up
children and parents about pedestrian injuries.
support for primary care staff. Silagy et al,'? in a separate
Towner et aPI found few studies that had analyzed re-
review, found that training had a measurable impact on
sults by occupational social class. Of those that did, some
professional performance.
found that the interventions were less successful among
Reviews have shown that the use of nicotine replace-
lower social classes." Some studies reported success in
ment therapy (nicotine gum or patches), can help in
targeting the lower social classes. For example, Colver et
smoking cessation interventions. IS However, patches
al" showed that pre-arranged personal home visits to
are expensive and in the UK are not available on NHS
iden tify specific targets for change in families living in a
prescription.
deprived area of Newcastle encouraged them to make
Connett and Stamler" have shown that interventions
changes in their homes that would be expected to re-
can be successfully carried out to reduce the incidence
duce the risk of childhood accidents. Because there may
of smoking in deprived groups. Their intensive medical
be a disproportionately low uptake by those at higher
treatment and education programme in the USA suc-
risk, it may be important to target such groups with ap-
ceeded in inducing extensive changes in the eating and
propriately designed interventions.
smoking habits of middle aged black and white Americans
of varying socio-economic backgrounds.
2. Accident prevention in older people
In their review, Oakley et aPI identified nine studies that 2. Cervical cancer
were considered to be sufficiently methodologically
sound and one meta-analysis. The principal finding Organized cervical cancer screening achieving a wide
from the research is that exercise, especially that which coverage of ages is effective at reducing risk." If wide
includes an element of balance training, reduces the risk coverage is assumed and uptake of high-risk (in particu-
of falls in older people. For example, Wolf et aP4 used lar inner city) groups is attained, then cervical smear
Tai Chi to improve balance as part of the 'Frailty and In- screening programmes may be effective in reducing
juries Co-operative Studies of Intervention Techniques' social class and regional inequalities in mortality. Marcus
(FICSIT) trials in the USA. et al 21 showed that prompts and incentives improved at-
tendance for follow-up appointments after women living
in a deprived urban community received an abnormal
Cancers smear result.
This section considers interventions aimed at reducing McAvoy and Raza" showed that a home visit with
the prevalence and incidence of cervical cancer, and support materials in relevant languages increased the
lung cancer (via smoking reductions). In the UK, in- attendance for cervical smears by Asian women in the
equalities exist in smoking behaviour and smoking- UK, though these groups are at lower risk of cervical
related deaths by social class," and there is a social class cancer than the UK population as a whole.
gradient in the incidence of and mortality from cervical There is evidence that women over the age of 65 would
cancer. 15 benefit from cervical and breast cancer screening."
Some of the age inequality in cervical and breast cancer
mortality may be avoidable by extending the upper age
1. Smoking
limit for the cervical and breast cancer screening pro-
A review by Sanders" found that health care settings are grammes in the UK beyond the age of 65.
a useful site for smoking cessation interventions and that
interventions can be given by a number of health care
Coronary heart disease (CHD)/stroke
professionals.
Brief advice from a GP to stop smoking in a general There exists a marked social class gradient in deaths
consultation can help a small (about 3%) but significant from CHD and stroke in the UK. 2 Furthermore, because
number of individuals to stop smoking and remain non- some health care professionals mistakenly assume that
smokers for at least a year. 16 Such advice can be improved treatments are less effective in older people, they use age
by offering follow-up appointments, health education rather than physiological status - age discrimination - to
and self-help booklets, concentrating on the short-term determine care." There are also inequalities by ethnicity.
as opposed to long-term benefits, negotiating a date to Death rates from CHD in people of South Asian origin
J Health Serv Res Policy Volume 1 Number 2 April 1996 95
A systematic review of the effectiveness of health service interventions Review article
living in the UK are about 40% higher than those of the Primary care screening should be used to identify and
white population and people of Afro-Caribbean origin target those who are at high risk.
have double the stroke mortality and many times greater
b) Cardio-vascular disease and stroke prevention in Afro-
rates of death associated with high blood pressure than
Caribbeans. Weight reduction and blood pressure control
the rest of the population.P
using drugs are both likely to reduce blood pressure
and hence the high rates of stroke in Afro-Carribeans."
1. CHD and stroke prevention in older people However, since lifestyle changes such as weight reduction
Ebrahim and Davey Smith" found strong evidence to are difficult to induce and maintain, blood pressure is
support the use of medical (drug) treatments for even more effectively controlled using drugs. Not all classes
mild degrees of hypertension in older people. The treat- of anti-hypertensive drugs may be equally effective in
ments are equally effective in relative terms at younger Mro-Caribbeans; drugs acting mainly on the renin-
and older ages up to the age of 80-85 years with absolute angiotensin system such as beta-blockers and ACE inhibi-
effects being far greater at older rather than younger tors may be less effective than low dose diuretics."
ages. Of single non-drug interventions, weight reduction Despite the fact that effective interventions such as
and exercise were found to be of value in lowering blood those described above are available to reduce CHD and
pressure. stroke risk in older people, Afro-Caribbean and Asian
The authors found the effectiveness of cholesterol ethnic groups and lower social classes, there is evidence
lowering using older cholesterol lowering agents such as that many people go undetected or are poorly managed
the fibrates to be dependent upon the level of risk. even when detected as being at high risk." Studies show-
Those at low overall risk of CHD were unlikely to derive ing success in tackling these problems include Stamler et
substantial benefits from cholesterol lowering by these al 30 who vigorously targeted an at-risk population in the
drugs and the authors recommend that widespread use USA to improve their access to hypertensive care. Tudor
of such drugs for cholesterol lowering in older people Hart et aPI found that intensive GP-based case finding
should not be promoted unless they are at particularly and vigorous follow-up in a deprived population im-
high risk of developing, or already have, CHD. The recent proved health outcomes.
West of Scotland pravastatin trial, however, has shown Gunnel and Smith'" in a review showed that coronary
substantial overall benefit in those at lower risk, al- artery bypass grafting (CABG) and angioplasty are effec-
though it is not clear what effect pravastatin has in older tiv~ at reducing distress and improving survival for peo-
people." Ebrahim and Davey Smith" found that very low ple with symptomatic CHD. However, there is some
fat diets may lower cholesterol levels, although the level evidence that in England, people in more deprived areas
of reduction is dependent upon compliance and severity have lower CABG procedure rates in relation to need
of the regimen imposed. than those living in more affluent areas with lower levels
Ebrahim and Davey Smith" found that whilst multiple of morbidity.'" Ensuring better access to CABG surgery
interventions among general and working populations for people with CHD in more deprived areas may there-
can modify risk factors, the changes achieved are rela- fore help reduce inequalities in death rates.
tively small, especially when compared to pharmacologi-
cal therapy.
Sexual health, HIV/AIDS and preventing
teenage pregnancy
2. CHD/stroke prevention in South Asians and
Mro-Caribbeans As HIV and other STDs are communicated by specific
patterns of risky behaviours including unprotected sex
McKeigue and Chaturvedi" reviewed the evidence on (vaginal and anal), or the sharing of needles, variations
preventing cardia-vascular disease in Afro-Caribbean exist by age, race, gender and sexual orientation." In
and Asian ethnic groups in Britain. the USA, minority groups are over-represented among
a) CHD and South Asians. McKeigue and Chaturvedi'" those with HIV.
found that raised death rates appear to be related to cen- There are inequalities in teenage pregnancy rates in
tral obesity (where a high proportion of body fat is young people by social class" and ethnicity" and the
deposited on the abdomen and trunk) and a higher young, lower social classes are more likely to suffer adverse
prevalence of insulin resistance in South Asians, in addi- consequences from early unintended pregnancies."
tion to the standard risk factors. Additionally, Hughes
et al 28 reported evidence that people with CHD from
1. Sexual health and HIV/ AIDS
an ethnic minority were diagnosed later in the disease
process. Since a high proportion of South Asians are The five recent reviews of this area34,37-4 0 comment on the
registered with a GP, primary care can be an important poor quality of the evaluative research in the area. Inter-
site for implementing CHD prevention strategies." ventions which aim to change community norms may be
McKeigue and Chaturvedi" suggest that health proma- a more effective and acceptable way to reduce high-risk
tion programmes can be enhanced if the range of facili- behaviours and prevent HIV than attempting to bring
ties in inner city practices can be improved with trained about change on an individual level." This approach has
personnel and access to bilingual staff or interpreters. been successfully applied with young people using the
96 J Health Serv Res Policy Volume 1 Number 2 April 1996
Review article A systematic review of the effectiveness of health service interventions
peer-led approach to education and with gay men III Cochrane and Sashidhararr" identified a number of
community mobilization programmes. areas in the UK where ethnic minorities suffer adverse
Effective sexual health promotion, particularly in mental health consequences. The authors note that
young people, involves the provision of clear information primary care appears to be failing as a pathway to spe-
on how STDs are and are not transmitted.tv" the provi- cialist care with referrals often more likely to be through
sion of condoms, skills building (in condom use and in the criminal justice system than GPs. Cochrane and
sexual negotiation), assertiveness training,34.37,41 and role Sashidharan"? recommend that better training should be
playing." Programmes which are based on formal social provided for GPs and other professionals to help them
psychological theory are found to be more effective than identify and treat psychological distress in South Asian
studies based on the assumption that knowledge trans- women.
lates directly into behavioural change or those with no Few good evaluations of interventions aimed at im-
theoretical basis.37.4O.41 proving mental health in deprived populations were
Interventions also need to be tailored to address identified. Some of the effective interventions used sim-
the needs of the target populations. For example, re- ple prompts (telephone calls and letters) to encourage
views have identified outreach as a successful means of attendance at mental health clinics." An intervention
providing health promotion to hard-to-reach groups which restructured the delivery of psychiatric rehabilita-
such as sex workers, injecting drug users, and men who tion to the homeless mentally ill was also found to be
have sex in public places. effective, reducing days spent homeless and improving
Jemmott et al 42 evaluated the effectiveness of an inner measures of mental health.f
city AIDS risk reduction programme targeted at young
black men in Philadelphia, PA, and found that 'cul- Pregnancy and childbirth
turally relevant learning' involving videos, games and
1. Social, financial and psychological support
exercises resulted in a reduction in those engaging in
during pregnancy and childbirth
risky behaviour. Behavioural interventions in the USA
involving AIDS education, cognitive-behavioural self- For those on a low income there is a close association
management and sexual-assertion training with high-risk between lack of support for health care costs and low
gay men led to reductions in the frequency of risky uptake of health care services.50 Social support, particu-
sexual behaviour (anal intercourse) and increased use of larly for mothers who are socially disadvantaged, can
refusal skills in white gay/bisexual men.P reduce the likelihood of adverse outcomes for the baby,
including child alfuse/neglect, severe nappy rash, otitis
2. Pregnancy prevention in young people media (middle ear infection), high blood pressure and
delayed appropriate immunization." Supported mothers
There is little reliable evidence of the effectiveness of
are also less likely to become pregnant again in the 18
special programmes of sex education over and above
months following childbirth. However, a review of eight
that which is routine in achieving reductions in preg-
RCTs including over 8000 women found that social
nancy rates. 40.41 Nonetheless, successful programmes
support for at-risk pregnant women was not associated
provide basic, accurate information about risks of unpro-
with any improvements in any medical outcomes of preg-
tected intercourse and methods of avoiding unprotected
nancy such as low birth weight or prematurity.50
intercourse," involved the young person, the family and
the community'? and aimed to improve young people's
2. Smoking during pregnancy
education, employment or economic situations."
Two reviews 44 •45 suggest that improving availability, ac- Since smoking reduces birthweight, smoking cessation
cessibility and acceptability of contraceptive services may programmes have a definite place in antenatal care.
improve effectiveness. Services should be confidential Trial results show that behavioural self-help strategies are
and well advertised; be developed in collaboration with more effective than advice and feedback in reducing
key statutory agencies, relevant voluntary groups and smoking in pregnancy. There is no evidence that coun-
community groups; should be broad-based; should be selling is effective.50
easily accessed outside school hours; should be staffed
by people trained to work with young people.'" should 3. Dietary modification in pregnancy
operate informally; and be shaped to meet the needs of
a) Folic acid supplements before and around the time of
the community served.
conception for women who are at increased risk of
giving birth to a child with neural tube defects reduce
Mental health
the risk of a recurrence by more than two-thirds.50 Ways
Mental health is more profoundly affected by socio- of ensuring that the intake of folic acid reaches the re-
economic factors than many other dimensions of'health." quired level within affordable, available and palatable
Health care interventions by themselves may be much food sources for each ethnic minority should be sought
less likely to have a significant impact on health inequali- within each country. This is a priority for public health
ties in this area. Indeed, policy makers might usefully tar- nutrition advice.
get some of their health budgets on social expenditure b) Other vitamin or mineral supplementation. Vitamin
(e.g. housing and employment) rather than treatment. D deficiency and subsequent hypocalcaemia can occur
J Health Serv Res Policy Volume 1 Number 2 April 1996 97
A systematic review of the effectiveness of health service interventions Review article
in women whose clothing leaves little exposed skin. Con- Community commitment
trolled trials in vulnerable populations showed a reduc-
A number of reviews l o,44,53 emphasised the importance of
tion in hypocalcaemia (low blood calcium levels) with
ensuring that the community in which the intervention
vitamin D supplements. Supplementation at the end of
was taking place supported the intervention, possibly
pregnancy should be considered in vulnerable groups
because of concern that focusing only on the individual
such as Asian women in Northern Europe."
ignored the more fundamental structural determinants
of social behaviour.
4. Breastfeeding
Multidisciplinary approaches
Efforts to provide social and psychological support may
increase the likelihood that mothers will breastfeed their A 'multidisciplinary approach' in which a number of
babies successfully. Research suggests that continued agencies were involved in the intervention can facilitate
personal support from an individual who is knowledge- the adoption of different strategies, the development
able about breastfeeding is most effective/" of improved information systems and harness more re-
sources. For example, Davidson et al 54 used a coalition of
local agencies to improve play areas, involve children
5. Screening for Chlamydia infection in high and adolescents in safe, supervised activities and to pro-
prevalence populations
vide injury and violence prevention education and safety
In the USA there are high rates of infection with equipment (e.g. bicycle helmets) at reasonable cost.
Chlamydia bacteria among young women, unmarried Ebrahim and Davey Smith" recommend the promotion
women and black women, as well as women from low of local health alliances as well as changes in national
socio-economic groups and those attending inner-eity and fiscal legislation to achieve reductions in smoking,
antenatal clinics. Congenital infection with Chlamydia dietary fat consumption, and the promotion of exercise
trachomatis is the most common cause of neonatal con- in attempts to reduce the risks of CHD and stroke. This
junctivitis, and there is a risk (3-8%) that an infant born is also a strong message emerging from the reviews of
to an infected mother will develop chlamydial pneumo- pregnancy prevention" and sexual health."
nia. If the prevalence of maternal infection among preg-
nant women is greater than 6% it is cost-effective to Multifaceted interventions
screen those at risk and to treat infected individuals."
Several successful programmes employed a combination
of interventions to improve the health of deprived
populations. For example, intensive 'stepped care' of
Characteristics of successful interventions hypertensives involved specialist treatment combined
aimed at improving the health of with attempts to improve access to the service."
disadvantaged groups Dannenberg et al 55 found that combining education
This section attempts to identify the characteristics of and legislation was more effective than education alone
interventions which have demonstrated success at im- in modifying children's behaviour in relation to bicycle
proving the health of disadvantaged groups. The charac- helmet use.
teristics have been found to be common to a number
of the interventions included in a review of 94 studies of Client-directed
interventions designed to reduce health inequalities," as interventions
well as the reviews contained within the previous section
of this paper.
Intensive approaches
Vigorous or intensive approaches have been shown to
Structured
improve the identification and subsequent effective
interventions Flexible
treatment of individuals, particularly those from deprived
interventions
populations. Levine and Bone," working in the USA,
used community health workers to screen, counsel,
follow-up and monitor people with high blood pressure,
focusing their efforts on young black males recruited
from the hospital casualty department. A similar ap-
proach was used by Stamler et al." Tudor Hart et aPI
found this approach useful in tackling a wider range of
health problems such as high blood pressure, smoking,
and obesity in a UK primary care setting. Professionally-
However, intensively targeting interventions is not directed interventions
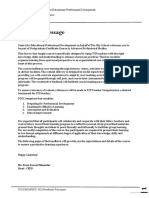
necessarily successful. 52 Figure Dimensions of face-to-face interventions.
98 J Health Serv Res Policy Volume 1 Number 2 April 1996
Review article A systematic review of the effectiveness of health service interventions
Face-to-face interactions trained outreach workers recruited from disadvantaged
communities to encourage appropriate use of ambula-
Many interventions involved face-to-face interactions
tory care services by other low-income families.
with individuals or small groups, often in an informal set-
ting. Broadly, these can be categorized in terms of two
general dimensions (Figure). The horizontal axis ranges Training those delivering the intervention
from structured interventions, such as a standardized A number of reviews highlighted the importance of
presentation to improve knowledge and attitudes to flex- training the individuals delivering the intervention,
ible interventions in the form of highly individualised whether they were non-professional volunteers or not.
meetings between clients and professionals. The vertical For example, Sanders" recommends training nurses, GPs
axis ranges from interventions tailored to the clients' and other health care professionals on smoking cessation
expressed preferences or established needs, to profes- techniques and Oakley et aPI emphasise the importance
sionally directed interventions. of training carers when they are running exercise classes
There is no clear evidence as to when it is appropriate for older people to help them maintain balancing skills.
to deliver an intervention to groups and when to deliver Freeborn et al 57 trained their outreach workers to
it to individuals. address a number of issues to improve the uptake of
ambulatory care services by families with low income.
Settings
Support materials
Interventions in a variety of settings have been shown to
be effective and it is likely that this depends on other Several interventions used educational materials such as
contextual factors. For example, many successful inter- booklets and videos. However, the impact of these mate-
ventions involved home visiting. However, these varied rials has rarely been assessed specifically. In some cir-
greatly by who was visited at home; by whom they were cumstances, educational materials may actually increase
visited; what was done during the visit; how long the inequalities in health. For example, Hibbard et al58 gave
home visits lasted and how frequently they occurred and an educational booklet to pregnant women and encour-
what they were trying to achieve. aged them to attend mothercraft classes and found
However, home visiting was not associated with an in- that women in higher social classes showed far greater
crease in uptake of breast cancer screening in an ethnic improvements in knowledge between early and late
minority group in one study." pregnancy than those in lower social classes.
Prior needs assessment to inform intervention Developing skills
design
Some of the interventions aimed to develop skills which
Some studies reported a form of needs assessmen t of the might facilitate the adoption of more health-promoting
target group to allow tailoring of the intervention. For activity. For example, Kelly et al 59 used group sessions to
example, Colver et aP3 identified hazards in family help disadvantaged young Afro-American women to rec-
homes before providing specific advice on preventing ognize personal triggers to risk-taking sexual behaviour,
domestic accidents. and to develop assertive techniques which would enable
them to reduce their risk of HIV infection.
Ensuring interventions are culturally
appropriate Provision of material support and resources
A related issue is the need for sensitivity to the culture of Some interventions offered material support in attempts
the target group. For example, McAvoy and Raza'" used to reduce barriers to the uptake of health services or to
an identifiably Muslim assistant to visit women of South increase participation in group activities. This included
Asian Muslim descent at home and produced videos and free transportation to antenatal and child health clinics
leaflets in relevant languages to improve uptake of cervi- for women living in poor rural areas. 50
cal screening in this group. However, Hoare et al 55 found Setting up a citizens' advice bureau in a primary
that home visiting of Bangladeshi and Pakistani women care or mental health day centre has been shown to help
by culturally matched linkworkers failed to improve the people in disadvantaged groups gain greater access to
uptake rates of breast screening. advice and resources, including welfare payments or
benefits. 51
The importance of the agent delivering the
intervention Provision of prompts and reminders to attend
The people who deliver the intervention may be as im- Several successful interventions used prompts or per-
portant as the intervention and its setting. Several suc- sonal reminders to encourage people to use services or
cessful interventions were carried out by non-professional keep appointments. PIanos and Glenwick" found that
volunteers, often recruited from the target population attendance rates for a scheduled mental health assess-
and trained to perform a task such as delivering a par- ment were higher with a telephone or postal reminder
ticular message. For example, Freeborn et al 57 used 1 or 2 days ahead.
J Health Serv Res Policy Volume 1 Number 2 April 1996 99
A systematic review of the effectiveness of health service interventions Review article
Discussion
The interventions delivered
The evidence summarized in the previous two main sec-
• Would an assessment of the target group's needs
tions has shown that there are a range of interventions
help shape the interventions appropriately?
which can be promoted through health services to re-
• Are the intended interventions acceptable, and cul-
duce health inequalities. Two clear messages emerge.
turally and educationally appropriate to the target
Firstly, if a health intervention is being used, there
group? (A pilot test might be advisable to assess
should be reasonable evidence that it has an impact on
this) .
health status. Secondly, having identified effective inter-
• Will members of the target group be involved in
ventions, care needs to be given to the way in which the
the design or development of the interventions?
intervention is delivered and the characteristics of an
• Will the interventions be fixed (delivered in the
implementation programme. These characteristics are
same way to everyone) or will they be flexibly
summarized in the Box.
delivered?
However, many of the interventions reviewed were
• Will the form and content of the intervention be
complex and involved a number of longitudinal, inter-
directed by the target group or by the provider?
personal and group interactions with people from de-
• How many component interventions will be
prived communities. It is often difficult to attribute
involved?
cause and effect from such evaluations, and it has been
• What opportunities will there be to reinforce the
suggested that a 'pluralistic' approach to evaluation is
in terventions?
needed for this form of intervention, incorporating both
qualitative and quantitative methods, as appropriate. 52 Setting and participants
Furthermore, only a few of the evaluations reviewed
• Is the setting accessible to and accepted by the
were of good quality and a number of common but
target audience?
avoidable problems with the design and execution of
• How homogeneous is the population of interest?
studies were identified, and are summarized below:
Would it be more appropriate to deliver the inter-
1. A number of studies gave only a limited description ventions to individuals or to groups? If to groups,
of the nature and content of the interventions used. what might be their best composition and size?
2. The sample sizes used were often too small.
Individual delivering the intervention
3. Many evaluations were conducted without any
attempt to identify a control group. • Who might be the most appropriate agent to de-
4. When a control group was included, many studies liver the interventions (e.g. health professional,
failed to carry out and/or report baseline measurements. teacher, community volunteer, trained peer)?
5. The follow-up periods used were often too short to • How credible are these people to the target group?
enable the potential value of an intervention to be assessed. How readily does the target group identify with
6. In some studies which randomly allocated people these people and what personal skills, training and
to different study groups, the randomisation was broken support might they need?
in the reporting of results.
Support materials/resources
In view of these points, care must be taken not to over-
• If the intervention requires the use of written or
analyse the study results in an attempt to extract
audiovisual materials what are the most appropriate
lessons for practice that are notjustified by the evidence.
materials (e.g. leaflets, videos, audiocassettes) con-
For example, although it might be tempting to draw con-
sidering the language abilities, literacy skills and
clusions about the relative effectiveness of different ap-
preferences of the target group?
proaches to increasing the uptake of cervical screening
• Would the provision of assistance with transport
among disadvantaged women, the relatively small number
and/or child care make it easier for members of
of studies, their heterogeneity and complexity would
the target group to attend the health care interven-
make any firm conclusions unreliable.
tion?
We did not systematically review the results of observa-
tional studies of health service interventions aimed to
Box Checklist of points to consider when designing
improve health in disadvantaged groups. This reflects
an intervention
both time constraints and the problems of attributing
changes in health outcomes to the interventions in ob-
servational study designs. In order to assess the effect of health coverage programmes for the poor uninsured,
excluding non-experimental designs, recent reviews in pre-natal care, pre-school use of preventive services, early
this area which did not exclude observational studies education, nutritional supplementation of children or
were examined.v" Of 98 papers in a major Dutch pregnant women, stress management, general preven-
review," were excluded because they did not fit at tive mass media and direct health education campaigns,
least one of the inclusion criteria and only three of the unemployment-related interventions, patient informa-
studies included in Bunton et al" were included in the tion leaflets and advocacy especially for ethnic minority
current review. groups. The results of evaluations of these interventions
The excluded studies examined interventions such as seem broadly in line with those reported in this review.
100 J Health Serv Res Policy Volume 1 Number 2 April 1996
Review article A systematic review of the effectiveness of health service interventions
Two population-wide programmes in the USA de- variations in the provision of services and in improving
signed to tackle the effects of poverty on growth, devel- health care for people who are poor, principally through
opment and education have been extensively evaluated free access to health care and attempts to ensure a more
and are worthy of mention. The Special Supplemental equitable distribution of health services.'" The provision
Food Programme for Women, Infants and Children of universal access to health care free at the point of
(WIC) was initiated in 1972 to improve the nutrition of delivery can itself be considered an intervention to re-
low-income women and children who had at least one duce variations in health. However, evidence also exists
nutritional risk factor. This provides packages of highly to show that, while removing financial barriers may be a
nutritious food and nutrition education, along with the necessary condition to improving equity, it is not in itself
provision of health services to low income nutritionally sufficient. 59
at-risk women who are pregnant or breast feeding and This review has shown that interventions to reduce
children up to the age of five. An evaluation of this pro- health inequalities can be evaluated using rigorous
gramme using a longitudinal study from 1980-1985 experimental methods such as randomized controlled
showed that there was a statistically significant correlation trials. Without such evaluation and monitoring, invest-
between the intensity of the WIC service and health- ments in such activities, whilst appearing to address this
related outcomes such as mean birthweight and reduc- important agenda, may be having little impact and be
tion in late fetal death, particularly in the poorest and better used in other ways. It is important that strategies
most high risk groups. 53 A recent meta-analysis of various developed to reduce inequalities are not assumed to
evaluations of the WIC programme estimated that pro- be having a positive impact simply because the aim is
viding the WIC programme to pregnant women reduced 'progressive' and so rigorous evaluations of promising
low birth weight and very low birth weight rates in disad- interventions are important.
vantaged groups by 25% and 44% respectively and would This review has concentrated only on interventions
pay for itself by savings in medical costs." which health services can implement alone or in collabo-
A second major welfare programme started in 1965 in ration with other agencies. Since it is likely that non-
the USA. Project Head Start provided pre-school chil- health service factors contribute most to health
dren and their families with education, health and social inequalities in developed countries, they are likely to
services. There have been several longitudinal studies have a crucial role to play in the reduction of inequalities
evaluating the effect of pre-school education which col- in health. Strategies available to tackle inequalities in
lectively appear to show short- and long-term benefits on health range from social and economic policy aimed at
cognitive and health-related outcomes. 55•56 Both these addressing the more fundamental inequalities in society
programmes have characteristics which have been iden- such as those of income distribution, to health care inter-
tified from the trials as being associated with success in ventions such as those included in this paper which
reducing variations in health, in particular their intensity essentially leave the system which generates the ine-
or targeting of those in need and their broad, multi- qualities intact and target health services at those at
disciplinary perspective including, for example, social greatest risk." The relative effectiveness and efficiency of
services, nutrition and health-related interventions. different approaches is an empirical question which re-
It should not be assumed that the general application quires more research; for example, to be in a position to
of an effective health care intervention will reduce in- estimate the proportion of the total variation in health
equalities. If, for example, uptake or effect differs by so- which could be reduced by each approach. In the ab-
cial group inequalities may actually widen. Experimental sence of comprehensive empirical evidence, the ultimate
studies in the areas of accident prevention" and the use choice of strategy is political.
of educational booklets for pregnant womerr" showed
greater impact in people from higher social classes. A
cross-sectional study examining the effect of an interven- Note
tion to increase immunization uptake in a region of the The full text of the review is available from the NHS Centre for Reviews
UK showed that although overall coverage for pertussis, and Dissemination at the University if York, UK.
diphtheria and measles immunization rose very signifi-
cantly, inequalities between deprived and affluent areas Acknowledgements
persisted or became wider." This highlights the impor-
tance of targeting interventions and evaluating their We are grateful for the advice and support given by George Davey Smith,
Louise Gunning-Scheppers, Jennie Popay, Margaret Whitehead,
impact. Annemieke Gepkens,Julie Glanville, Sally Baker and Paula Press.
Community development programmes aimed at re- The NHS Centre for Reviews and Dissemination is funded by the
ducing inequalities in health may also be effective. How- NHS Executive and the Health Departments of Scotland, Wales and
Northern Ireland; a contribution to the Centre is also made by the
ever, since few of these have been evaluated, they are University of York. The views expressed in this publication are those of
not dealt with in this review. the authors and not necessarily those of the NHS Executive or the Health
Departments of Scotland, Wales and Northern Ireland.
Conclusions References
1. Phillimore P, Beattie A, Townsend P. Widening inequality
Significant progress has been made since the establish- of health in northern England, 1981-91. British Medical
ment of the NHS in the UK in reducing the geographical Journal 1994; 308: 1125-1128.
J Health Serv Res Policy Volume 1 Number 2 April 1996 101
A systematic review of the effectiveness of health service interventions Review article
2. Department of Health. Variations in Health: what can the 22. McAvoy B R, Raza R. Can health education increase the
Departmentof Health and the NHS do? A report produced uptake of cervical smear testing among Asian women?
by the Variations Sub-Group of the Chief Medical British Medical Journal 1991; 302: 333-336.
Officer's Health of the Nation Working Group. London: 23. Medical Research Council. The Health of the UK'sElderly
Department of Health, October 1995. People. MRC Topic Review. London, MRC 1994; Ch 10.
3. MackenbachJ P, van de Mheen H, Stronks K. A 24. Fotherby M D, Harper G D, Potter J F. Management of
prospective cohort study investigating the explanation of hypertension in elderly patients. British MedicalJournal
socio-economic inequalities in health in the Netherlands. 1992; 305: 750-752.
Social Science and Medicine 1994; 38: 299-308. 25. McKeigue P, Chaturvedi N. Epidemiology and Control of
4. Arblaster L, Entwistle V, Lambert M, Forster M, Sheldon Cardiovascular Disease in South Asians and Afro-
T A and Watt I. Reviewof the Research on theEffectiveness of Caribbeans. In: Ahmad W, Sheldon T A, Stuart a (eds).
Health Service Interventions to Reduce Variations in Health. Ethnicity and Health: Reviewsof literature and guidance
CRD Report 3. York: NHS Centre for Reviews and for purchasers in the areasof cardiovascular disease, mental
Dissemination, University of York, 1995. health and haemoglobinopathies. CRD Report 5. York: NHS
5. Department of Health. Health of the Nation: a strategy for Centre for Reviews and Dissemination, University of York
health in England. London: HMSO, 1992. 1966.
6. FeinsteinJ S. The relationship between socioeconomic 26. Ebrahim S, Davey Smith G. Health promotion for coronary
status and health: a review of the literature. Millbank heart disease and stroke prevention in olderpeople. Report
Quarterly 1993; 71: 279-322. prepared for the York NHS Centre for Reviews and
7. Benzeval M,Judge K, Whitehead M (eds). Tackling Dissemination, 1995 (unpublished).
Inequalities in Health: an agendafor action. London: King's 27. ShepherdJ, Cobbe S M, Ford I, Isles C G, Lorimer A R,
Fund,1995. MacFarlane P W et al. Prevention of coronary heart
8. Gepkins A, Gunning-Schepers LJ, Interventies ter disease with pravastatin in men with
verminderingvan sociaal-economische gezondheidsverschillen hypercholesterolemia. The New EnglandJournal of
(Interventions to address socio-economic inequalitiesin health). Medicine 1995; 333: 1301-1307.
Amsterdam: Institute of Social Medicine, University of 28. Hughes L 0, Ravel U, Rafferty E B. First myocardial
Amsterdam, 1993 (unpublished). infarctions in Asian and white men. British Medical
9. Bunton R, Burrows R, Gillen K, Muncer S. Interventions to Journal 1989; 298: 1345-1350.
promote health in economically deprived areas: a critical review 29. Smith W C, Lee AJ, Crombie I K, Tunstall-Pedoe H.
of the literature. Newcastle: NHS Executive, Northern and Control of blood pressure in Scotland: the rule of halves.
Yorkshire Region, 1994. British Medical Journal 1990; 300: 981-983.
10. Towner E, Dowswell T, Simpson G,Jarvis S. Preventing 30. Stamler R, Hardy RJ, Payne G H, Tyroler H A, Tung B,
unintentional injuries in childhood and adolescence. CRD Newman B et al. Educational level and 5-year all-eause
Report. York: NHS Centre for Reviews and mortality in the hypertension detection and follow-up
Dissemination, University of York (in press). program. Hypertension Detection and Follow-up
11. Oakley A, Cryer C, France-Dawson M, Doyle Y, Fullerton Program 1987; 9: 641-646.
D, Rice J et al. Review ofEffectiveness of Health Promotion 31. Tudor HartJ, Thomas C, Gibbons, B, Edwards C, Hart
Interventions to PreventAccidentsin OlderPeople. CRD M,JonesJ et al. Twenty five years of case finding and
Report. York: NHS Centre for Reviews and audit in a socially deprived community. British Medical
Dissemination, University of York (in press). Journal 1991; 302: 1509-1513.
12. Downing C. Evaluation of the impact and penetration of a 32. Gunnell D, Smith L. The invasive managementafischaemic
children's traffic club. Paper to Second International heart disease. Bristol: Health Care Evaluation Unit,
Conference on Road Safety. Groningen, 1987. University of Bristol, 1994;
13. Colver A F, Hutchinson P J,Judson E C. Promoting 33. Ben-Shlomo Y, Chaturvedi N. Access to health care
children's home safety. British Medical Journal 1982; provision in the UK: does where you live affect your
285: 1177-1180. chances of getting a coronary artery bypass graft?
14. Wolf S L, Kutner N G, Green R C, McNeely E. The Journal of Epidemiology and Community Health 1995;
Atlanta FICSIT study: Two exercise interventions to 49: 200-205.
reduce frailty in elders. Journal of the American 34. Aggleton P. Sexual Behaviour and HIV/ AIDS. A Review of
Geriatrics Society 1993; 41: 341-343. the effectiveness of health education and healthpromotion.
15. OPCS. RegistrarGeneral's DecennialSupplementon Utrecht: Dutch Centre for Health Promotion and Health
OccupationalMortality 1979-83. London: HMSO, 1986. Education, 1994.
16. Sanders D. Smoking Cessation Interventions: is patient 35. Garlick R, Ineichen B, Hudson F. The UPA score and
educationeffective? A Review of the Literature. London: teenage pregnancy. Public Health 1993; 107: 135-139.
London School of Hygiene and Tropical Medicine, 1992. 36. Brown S S, Eisenberg L. The best intentions: Unintended
17. Silagy C, Lancaster T, Gray S, Fowler G. Effectiveness of pregnancy and the well-being of children and families.
training health professionals to provide smoking Washington DC: National Academic Press, 1995.
cessation interventions: systematic review of randomised 37. FisherJ D, Fisher W A. Changing AIDS risk behavior.
controlled trials. Quality in Health Care 1994; 3: 193-198. Psychological Bulletin 1992; 111: 455-474.
18. Ling TangJ, Law N, Wald N. How effective is nicotine 38. HollandJ, Arnold S, Fullerton D, Oakley A, Hart G.
replacement therapy in helping people to stop smoking? Review ofEffectiveness of Health Promotion Interventionsfor
British Medical Journal 1994; 308: 21-26. Men who have Sex with Men. London: Social Science
19. ConnettJ E, Stamler J. Responses of black and white Research Unit, 1994.
males to the special intervention program of the 39. Oakley A, Fullerton D, HollandJ, Arnold A, Hickey D,
Multiple Risk Factor Intervention Trial. American Heart Kelley P et al. Towards Effective Intervention. a critical
Journal 1984; 108: 839-849. evaluation of HIV prevention and sexual health interventions.
20. Austoker J. Screening for cervical cancer. British Medical London: Social Science Research Unit, 1994a.
Journal 1994; 309: 241-248. 40. Oakley A, Fullerton D, HollandJ, Arnold A, France-
21. Marcus A C, Crane L A, Kaplan C P, Reading A E, Savage Dawson M, Kelley P et al. Young People and Sexual Health:
E, GunningJ et al. Improving adherence to screening a review of the effectiveness afinterventions. London: Social
follow-up among women with abnormal Pap smears. Science Research Unit, 1994b.
Medical Care 1992; 30: 216-229. 41. Kirby D. A review of educationalprograms designed to reduce
102 J Health Serv Res Policy Volume 1 Number 2 April 1996
Review article A systematic review of the effectiveness of health service interventions
sexual risk-takingbehauiors among school-age youth in the 1988 through 1991. AmericanJournal of Public Health
United States. Santa Cruz, Ca: ETA Associates, 1995. 1994; 84: 580-586.
42. JemmottJ B,Jemmott L S, Fong G T. Reduction in HIV 55. Dannenberg A L, Gielen A C, Beilenson P L, Wilson M F,
risk-associated sexual behaviours among black male Joffe A. Bicycle helmet laws and educational campaigns:
adolescents: Effects of an AIDS prevention intervention. and evaluation of strategies to increase children's helmet
American Journal of Public Health 1992; 82: 372-377. use. AmericanJournal of Public Health 1993; 83: 667--674.
43. KellyJ A, St Lawrence J S, Stevenson L y, Hauth A C, 56. Hoare T, Thomas C, Biggs A, Booth M, Bradley S,
Kalichman S C, Diaz YE et al. Community AIDS/HIV Friedman E. Can the uptake of breast screening in Asian
risk reduction: the effects of endorsements by popular women be increased: a randomized controlled trial of a
people in three cities. American Journal of Public Health linkworker intervention. Journal of Public Health
1992;82: 1483-1489. Medicine 1994; 16: 179-185.
44. Peach E, Harris J, Bielby E: Teenage Pregnancy. - A 57. Freeborn D K, MulloolyJ P, Colombo T, Burnham V. The
communityissue. A literature review. Report for the effect of outreach workers' services on the medical care
Yorkshire Collaborating Centre for Health Services utilization of a disadvantaged population. Journal of
Research. Leeds: Nuffield Institute for Health, University Community Health 1978; 3: 306--320.
of Leeds, 1994. 58. Hibbard B M, RobinsonJ 0, PearsonJ F, Rosen M,
45. Peckham S, Ingham R, Berrington A, Diamond 1. Teenage Taylor A. The effectiveness of antenatal education.
pregnancy: Prevention and programmes. Institute fur Health Health Education Journal 1979; 38: 39-46.
Policies. Southampton: University of Southampton, 1995 59. KellyJ A, Murphy D A, Washington C D, Wilson T S, Koob
(Unpublished) . J J, Davis D Ret al. The effects of HIV/ AIDS intervention
46. Carr Hill R A, Hardman G, Martin S, Peacock S, groups for high-risk women in urban clinics. American
Sheldon T A, Smith P. A Formula fur DistributingNHS Journal of Public Health 1994; 84: 1918-1922.
RevenuesBased on SmaUArea Use. Occasional Paper. York: 60 Olds D L, Henderson C R, Kitzman H. Does prenatal
Centre For Health Economics, University of York, August and infancy nurse home visitation have enduring effects
1994. on qualities of parental caregiving and child health at 25
47. Cochrane R, Sashidharan S P. Mental Health and Ethnic to 50 months oflife? Paediatrics 1994; 93: 89-98.
Minorities: a review of literature and implications for 61. ParisJ M G, Player D. Citizen's advice in general
services. In: Ahmad W, Sheldon T A, Stuart 0 (eds) practice. British Medical Journal 1993; 306: 1518-1520.
Ethnicity and Health: Reviewsof literature and guidancefur 62. Beattie A. Evaluating generic community interventions.
purchasers in the areasof cardiovascular disease, mental health In: PopayJ, Young A (eds). Reducing accidental death and
and haemoglobinopathies. CRD Report 5. York: NHS Centre injury in children. Salford: Public Health Research and
for Reviews and Dissemination, University of York 1996. Resource Centre and Manchester Public Health
48. PIanos R, Glenwick D. The effects of prompts on a Resource Centre, 1993.
minority children's screening attendance at a community 63. Rush D, Sloan N, LeightonJ et al. The National WIC
mental health center. Child and Family Behaviour Evaluation: evaluation of the Special Supplemental Food
Therapy 1986; 8: 5-13. Programme for Women, Infants and Children. V -
49. Wasylenki D A, Goering P N, Lemire D, Lindsey S, longitudinal study of pregnant women. American
Lancee W. The hostel outreach programme: assertive Journal of Clinical Nutrition 1988; 48: 439-483.
case management for homeless mentally ill persons. 64. Avruch S, Cackly A P. Savings achieved by giving WIC
Hospital and Community Psychiatry 1993; 44: 848-853. benefits to women prenatally. Public Health Reports
50. Enkin M W, Keirse MJ N C, Renfrew MJ, NeilsonJ P, 1995; 110: 27-34.
Crowther C (eds). Pregnancy and Childbirth module. In: 65. Lazar I, Darlington R B, Murray H, Royce J, Snipper A.
The Cochrane Database of Systematic Reviews (database Lasting effects of early education: a report from the
on disc and CD-Rom), The Cochrane Collaboration, Consortium of Longitudinal Studies. Monographs of the
Issue 2. Oxford: Update Software; 1995. (Available from Society for Research in Child Development 1982; 47: 2-3.
BMJ Publishing Group, London.) 66. Schweinhart LJ, Weikart D P. Success by empowerment-
51. Levine D M, Bone L. The impact of a planned health the High Scope Perry Preschool Study through age 27.
education approach on the control of hypertension in a Young Children 1993; 49: 54-58.
high risk population. Journal of Human Hypertension 67. Reading R, Colver A, Openshaw S,Jarvis S. Do
1990; 4: 317-321. interventions that improve immunisation uptake also
52. Marsh G N, Channing D M. Narrowing the health gap reduce social inequalities in uptake? British Medical
between a deprived and an endowed community. British Journal 1994;308: 1142-1144.
Medical Journal 1988; 296: 173-176. 68. Le GrandJ, Winter D, Woolley F. The National Health
53. FinneyJ W, Christopherson E R, Frisman P C, Kalnins Service; safe in whose hands? In: The State of Welfare.
I V, Maddox J E, Peterson L et al. Society of Pediatric HillJ (ed). Oxford: Clarendon, 1990.
Psychology Task Force Report: Pediatric psychology and 69. Short P F, Lefkowitz DC. Encouraging preventive
injury control. Journal of Pediatric Psychology 1993; services for low-income children. The effect of
18: 499-526. expanding Medicaid. Medical Care 1992; 30: 766--780.
54. Davidson L L, Durkin M S, Kuhn L, O'Connor P, Barlow 70. Wilkinson R G. Variations in health: The cost of
B, Heagarty M C. The impact of the Safe Kids/Healthy government timidity. British Medical Journal 1995;
Neighborhoods Injury Prevention Program in Harlem, 311: 1177-1178.
J Health Serv Res Policy Volume 1 Number 2 April 1996 103
You might also like
- Hide Tanning PDF - FINAL7.23Document32 pagesHide Tanning PDF - FINAL7.23Kevin100% (1)
- Employee Safety Training Matrix Template ExcelDocument79 pagesEmployee Safety Training Matrix Template Excelشاز إياسNo ratings yet
- Strategy Implementation, Evaluation and ControlDocument6 pagesStrategy Implementation, Evaluation and Controlbonny MishNo ratings yet
- Population HealthDocument444 pagesPopulation HealthC R D100% (3)
- Brand Awareness Questionnaire SampleDocument2 pagesBrand Awareness Questionnaire SampleYogesh Sangani77% (13)
- Rapid Prototyping and ToolingDocument2 pagesRapid Prototyping and ToolingelangandhiNo ratings yet
- Natural Remedies For Gout (High Uric Acid) - Natural Gout TreatmentDocument12 pagesNatural Remedies For Gout (High Uric Acid) - Natural Gout Treatmentkapoor_mukesh4uNo ratings yet
- Bombardier Zefiro Technical Description enDocument15 pagesBombardier Zefiro Technical Description ennickerlesstezla100% (1)
- University of Tennessee Religious ExemptionDocument3 pagesUniversity of Tennessee Religious ExemptionDonnaNo ratings yet
- 17.321.2687 Ni Komang Sri WahyuniDocument19 pages17.321.2687 Ni Komang Sri Wahyunigekayu sartikaNo ratings yet
- Community Health Factors and Health DisparitiesDocument7 pagesCommunity Health Factors and Health Disparitiesshreeguru8No ratings yet
- Confronting Health Inequity - The Global DimensionDocument5 pagesConfronting Health Inequity - The Global Dimensionmanique_abeyrat2469No ratings yet
- Foster, Peggy. Inequalities in HealthDocument5 pagesFoster, Peggy. Inequalities in HealthMuhammad NasherNo ratings yet
- Ebb PDFDocument12 pagesEbb PDFMonica TanNo ratings yet
- Östlin - Paying Attention To GenderDocument6 pagesÖstlin - Paying Attention To GendermariaconstanzavasqueNo ratings yet
- Disparities Interim Report 2Document33 pagesDisparities Interim Report 2Lydia WanjikuNo ratings yet
- Strengthening Health Information Systems To Address Health Equity ChallengesDocument16 pagesStrengthening Health Information Systems To Address Health Equity ChallengesAhlidin S.No ratings yet
- Lin - Gender SensitiveDocument8 pagesLin - Gender SensitivemariaconstanzavasqueNo ratings yet
- Gha 9 29329Document19 pagesGha 9 29329Bahtiar AfandiNo ratings yet
- Health Indicators: Ple 2000 & Healthy People 2010) Were MoreDocument5 pagesHealth Indicators: Ple 2000 & Healthy People 2010) Were MoreSyamsir RusdinNo ratings yet
- The Changing Demographic Profile of Eating Disorder Behaviors in The Community 2.23.16 PMDocument9 pagesThe Changing Demographic Profile of Eating Disorder Behaviors in The Community 2.23.16 PMShera LopezNo ratings yet
- Health Outcome in India An Analysis of Multidimensional InequalityDocument8 pagesHealth Outcome in India An Analysis of Multidimensional InequalityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Global HealthDocument3 pagesGlobal HealthDinda ElahmadiNo ratings yet
- Ill-Health and Poverty A Literature Review On Health in Informal SettlementsDocument10 pagesIll-Health and Poverty A Literature Review On Health in Informal Settlementsc5m07hh9No ratings yet
- Articulo Salud InglesDocument10 pagesArticulo Salud InglesmaryNo ratings yet
- Running Head: LITERATURE REVIEW 1Document7 pagesRunning Head: LITERATURE REVIEW 1Seymour WardNo ratings yet
- Social Epidemiology: Questionable Answers and Answerable QuestionsDocument4 pagesSocial Epidemiology: Questionable Answers and Answerable QuestionsvictorNo ratings yet
- Jurnal B.inggrisDocument7 pagesJurnal B.inggrishellda putri arieskaNo ratings yet
- Gender Promotion UpdatedDocument3 pagesGender Promotion Updatedkudabo oluwatosinNo ratings yet
- Understanding Population Health Terminology: University of WisconsinDocument24 pagesUnderstanding Population Health Terminology: University of WisconsinKizer Roselynn JamiNo ratings yet
- Social Epidemiology: Questionable Answers and Answerable QuestionsDocument4 pagesSocial Epidemiology: Questionable Answers and Answerable QuestionsAsad MotenNo ratings yet
- Nursing ResearchDocument15 pagesNursing Researchsubhashreepal13No ratings yet
- The Impact of Cash Transfers On Social Determinants of Health and Health Inequalities in Sub-Saharan Africa: A Systematic ReviewDocument22 pagesThe Impact of Cash Transfers On Social Determinants of Health and Health Inequalities in Sub-Saharan Africa: A Systematic Reviewlight1plusNo ratings yet
- Defining Cultural Competence - A Practical Framework For Addressing RacialEthnic Disparities in Health and Health CareDocument10 pagesDefining Cultural Competence - A Practical Framework For Addressing RacialEthnic Disparities in Health and Health CareMaulidza SiltaNo ratings yet
- Universal Health Coverage in Latin America 3: SeriesDocument9 pagesUniversal Health Coverage in Latin America 3: SeriesEgi NabilaNo ratings yet
- Nimhd Strategic Plan 2021 2025Document38 pagesNimhd Strategic Plan 2021 2025jeanbourgeatNo ratings yet
- Public Health Dissertation TitlesDocument7 pagesPublic Health Dissertation TitlesWriteMyPaperPleaseSingapore100% (1)
- Health Seeking BehaviourDocument27 pagesHealth Seeking BehaviourRommel IrabagonNo ratings yet
- Zayyana Musa T-PDocument34 pagesZayyana Musa T-PUsman Ahmad TijjaniNo ratings yet
- Journal Reading 5Document6 pagesJournal Reading 5Ronaly Angalan TinduganNo ratings yet
- What Is "Community Health Examining The Meaning of An Evolving Field in Public HealthDocument4 pagesWhat Is "Community Health Examining The Meaning of An Evolving Field in Public Healthد.شيماءسعيدNo ratings yet
- Global Health Initiatives 2007 enDocument32 pagesGlobal Health Initiatives 2007 enChristian Anthony CullarinNo ratings yet
- Jurnal KedokteranDocument18 pagesJurnal KedokteranelvandryNo ratings yet
- 0rder 335 - Policy and Advocacy For Population HealthDocument6 pages0rder 335 - Policy and Advocacy For Population Healthjoshua chegeNo ratings yet
- Socio-Economic Inequalities in Health and Health Service Use Among Older Adults in India - Results From The WHO Study On Global AGEing and Adult Health SurveyDocument10 pagesSocio-Economic Inequalities in Health and Health Service Use Among Older Adults in India - Results From The WHO Study On Global AGEing and Adult Health SurveyAnindita BalaganesanNo ratings yet
- Utility and Limitations of Measures of Health Inequities A Theoretical PerspectiveDocument9 pagesUtility and Limitations of Measures of Health Inequities A Theoretical PerspectiveStephanyNo ratings yet
- Understanding How Discrimination Can Affect HealthDocument15 pagesUnderstanding How Discrimination Can Affect HealthNna HsnNo ratings yet
- Assignment On Public Health CareDocument14 pagesAssignment On Public Health CareImpatient KashemNo ratings yet
- American Thoracic Society Statement On Research Priorities in Respiratory NursingDocument8 pagesAmerican Thoracic Society Statement On Research Priorities in Respiratory NursingRESCATEURNo ratings yet
- Marmot y Allen (2014)Document7 pagesMarmot y Allen (2014)Hospitales Federales de Referencia CCINSHAENo ratings yet
- A Vital Direction For Health and Health Care: Addressing Social Determinants of Health and Health DisparitiesDocument16 pagesA Vital Direction For Health and Health Care: Addressing Social Determinants of Health and Health DisparitiesEgi NabilaNo ratings yet
- Town and Gown Collaboration: A Practical PerspectiveDocument10 pagesTown and Gown Collaboration: A Practical PerspectivemperezfresnoNo ratings yet
- Sociodemographic Factors Related To Self-Medication in SpainDocument2 pagesSociodemographic Factors Related To Self-Medication in SpainNovita SugianthiNo ratings yet
- Governance of Healthcare System: Frameworks For Gender Mainstreaming Into Public HealthDocument10 pagesGovernance of Healthcare System: Frameworks For Gender Mainstreaming Into Public HealthFika Nur FadhilahNo ratings yet
- Primaryhealthcareandthesocial Determinantsof Health EssentialDocument5 pagesPrimaryhealthcareandthesocial Determinantsof Health Essential98b5jc5hgtNo ratings yet
- Comment: Vs Failure of Implementation), Which Can Provide UniqueDocument2 pagesComment: Vs Failure of Implementation), Which Can Provide UniquedanielNo ratings yet
- Annotated Biblography 1Document6 pagesAnnotated Biblography 1api-704699003No ratings yet
- Priorities, 3rd Edition: ReviewDocument14 pagesPriorities, 3rd Edition: ReviewNatasha AlbaShakiraNo ratings yet
- Ananotaed BibliographyDocument12 pagesAnanotaed BibliographyElvis Rodgers DenisNo ratings yet
- Concepts in Public Health and Preventive MedicineDocument16 pagesConcepts in Public Health and Preventive MedicineMohammed AlwardiNo ratings yet
- Prevalence of Lower Urinary Tract Symptoms and Social Determinants in Primary Care Users in BrazilDocument8 pagesPrevalence of Lower Urinary Tract Symptoms and Social Determinants in Primary Care Users in BrazilBandac AlexandraNo ratings yet
- Rainbow Grade R BIG Book 1 2015 ResizedDocument22 pagesRainbow Grade R BIG Book 1 2015 ResizedLaurelleNo ratings yet
- A Three-Stage Approach To Measuring Health Inequalities and InequitiesDocument13 pagesA Three-Stage Approach To Measuring Health Inequalities and Inequitiessean8phamNo ratings yet
- Measures To Protect Health Workers From Exposure To Infectious DiseasesDocument20 pagesMeasures To Protect Health Workers From Exposure To Infectious Diseasesk ucheNo ratings yet
- Conceptual Models For Pop Health ArticleDocument6 pagesConceptual Models For Pop Health ArticleChantal CarnesNo ratings yet
- Baidin2021 Article HowSelf RatedIsSelf RatedHealtDocument22 pagesBaidin2021 Article HowSelf RatedIsSelf RatedHealtGabriel MacielNo ratings yet
- Reducing Racial/Ethnic Disparities in Reproductive and Perinatal Outcomes: The Evidence from Population-Based InterventionsFrom EverandReducing Racial/Ethnic Disparities in Reproductive and Perinatal Outcomes: The Evidence from Population-Based InterventionsArden HandlerNo ratings yet
- Worksheet GlobeDocument1 pageWorksheet GlobeJolens VelasquezNo ratings yet
- Civil Engineering MCQ'sDocument1 pageCivil Engineering MCQ'sNISHIKANTA MONDALNo ratings yet
- Boss DD-6Document28 pagesBoss DD-6Justin Alexander SanzonENo ratings yet
- TranscriptDocument1 pageTranscriptGursharanjit SinghNo ratings yet
- Hostel Standard and Safety MeasuresDocument16 pagesHostel Standard and Safety MeasuresSadiya IqbalNo ratings yet
- Food Photographs Practical Guidelines II Development and Use of Photographic Atlases For Assessing Food Portion SizeDocument7 pagesFood Photographs Practical Guidelines II Development and Use of Photographic Atlases For Assessing Food Portion SizemmmdeandradeNo ratings yet
- Government SyllabusDocument3 pagesGovernment Syllabusapi-100383549No ratings yet
- Traffic Monitoring SystemDocument16 pagesTraffic Monitoring Systemankit kumarNo ratings yet
- Garmin GNC 250xl Gps 150xlDocument2 pagesGarmin GNC 250xl Gps 150xltordo22No ratings yet
- Reynald Hernandez: ExperienceDocument2 pagesReynald Hernandez: ExperienceRey HernandezNo ratings yet
- Avamar - ADS Data Erasure-YES - I Understand All Data Will Be Lost by Performing This Procedure!Document30 pagesAvamar - ADS Data Erasure-YES - I Understand All Data Will Be Lost by Performing This Procedure!dansegui.mir4No ratings yet
- A View From Elkab The Tomb and Statues oDocument87 pagesA View From Elkab The Tomb and Statues oBeatriz FélixNo ratings yet
- Program Orientation HandoutsDocument125 pagesProgram Orientation Handoutsapi-391214898No ratings yet
- What Is A CodebookDocument5 pagesWhat Is A CodebookAxmed YaasiinNo ratings yet
- Arahan Dan Soalan Tugasan Jkp513e417e Sa 20222023Document4 pagesArahan Dan Soalan Tugasan Jkp513e417e Sa 20222023skblueNo ratings yet
- DBMS - Lab CAT2 Code SWE1001 SLOT L47+48 DATE 16/10/19Document2 pagesDBMS - Lab CAT2 Code SWE1001 SLOT L47+48 DATE 16/10/19msroshi madhuNo ratings yet
- Finalizing The Accounting ProcessDocument2 pagesFinalizing The Accounting ProcessMilagro Del ValleNo ratings yet
- ExcaDrill 45A DF560L DatasheetDocument2 pagesExcaDrill 45A DF560L DatasheetИгорь ИвановNo ratings yet
- Unit 2Document42 pagesUnit 2Kalaiselvan PunniyamoorthyNo ratings yet
- Novena To Our Lady Queen of PeaceDocument4 pagesNovena To Our Lady Queen of PeaceGraciedion MediaNo ratings yet
- Line-And-Staff Organizations - Examples, Advantages, Manager, Type, Company, Disadvantages, BusinessDocument4 pagesLine-And-Staff Organizations - Examples, Advantages, Manager, Type, Company, Disadvantages, BusinessSangram PradhanNo ratings yet
- PGCC 2022 HandbookDocument17 pagesPGCC 2022 HandbookhasnainNo ratings yet