You might also like
- Drug study highlights Allegra's mechanism, indications, and nursing responsibilitiesDocument1 pageDrug study highlights Allegra's mechanism, indications, and nursing responsibilitiesBlitz KriegNo ratings yet
- Drug Study FinalDocument5 pagesDrug Study FinalJackie Ann Marie DapatNo ratings yet
- Amlodipine CPDocument2 pagesAmlodipine CPRose EchevarriaNo ratings yet
- IsoketDocument2 pagesIsoketJaessa FelicianoNo ratings yet
- DRUG LactuloseDocument1 pageDRUG LactuloseJona Phie Domingo MonteroNo ratings yet
- DS (Fenofibrate)Document5 pagesDS (Fenofibrate)Mary April MendezNo ratings yet
- Drug StudyDocument4 pagesDrug Studyw dNo ratings yet
- Lui Sh-Colored Lips and Finger Nails Blur Red VisionDocument1 pageLui Sh-Colored Lips and Finger Nails Blur Red VisionMagdayao Romamea100% (1)
- DS (Calcium + Vit. D)Document6 pagesDS (Calcium + Vit. D)Mary April MendezNo ratings yet
- Drug Study Table 3Document5 pagesDrug Study Table 3Juliet De GuzmanNo ratings yet
- Check The Physician's Observe and Follow The 14 Warn The Mother AboutDocument2 pagesCheck The Physician's Observe and Follow The 14 Warn The Mother AboutJust nowNo ratings yet
- Drug Study ON Atropine Sulfate: Maa Tripura College of Nursing, Jhabua (M.P.)Document3 pagesDrug Study ON Atropine Sulfate: Maa Tripura College of Nursing, Jhabua (M.P.)amitNo ratings yet
- Verapamil HCLDocument3 pagesVerapamil HCLMae Ann Bueno CastillonNo ratings yet
- Insulin Mechanism of Action and Nursing ResponsibilitiesDocument7 pagesInsulin Mechanism of Action and Nursing ResponsibilitiesGrape JuiceNo ratings yet
- Drug SDocument2 pagesDrug SJane CasiquinNo ratings yet
- Virtual Clinical Duty Daily RequirementsDocument7 pagesVirtual Clinical Duty Daily RequirementsEdgie FabreNo ratings yet
- HYOSCINEDocument1 pageHYOSCINEzyr2189No ratings yet
- NafarinDocument2 pagesNafarinianecunar100% (2)
- NeoblocDocument2 pagesNeoblocianecunar100% (2)
- EtoricoxibDocument7 pagesEtoricoxibsatwika28100% (1)
- Sal But AmolDocument2 pagesSal But AmolKay MirandaNo ratings yet
- Drug study cilostazol intermittent claudicationDocument2 pagesDrug study cilostazol intermittent claudicationart_mutantNo ratings yet
- F. Case Study Thesis-Drug Study (Revised)Document5 pagesF. Case Study Thesis-Drug Study (Revised)Lopirts NiganiNo ratings yet
- Felodipine CefuroximeDocument3 pagesFelodipine CefuroximecotyboyNo ratings yet
- PrednisoloneDocument2 pagesPrednisoloneKatie McPeekNo ratings yet
- UnasynDocument1 pageUnasynrachieeeNo ratings yet
- Filgrastim Boosts Neutrophil Recovery After ChemotherapyDocument3 pagesFilgrastim Boosts Neutrophil Recovery After ChemotherapyKyla Barrera TabungarNo ratings yet
- TramadolDocument1 pageTramadolAi RouNo ratings yet
- Drug Study ICUDocument5 pagesDrug Study ICUEcko MoawiaNo ratings yet
- SalmeterolDocument2 pagesSalmeterolapi-3797941No ratings yet
- Enalapril MaleateDocument3 pagesEnalapril MaleatelichunghkNo ratings yet
- Nifedipine and Prednisone Drug StudyDocument5 pagesNifedipine and Prednisone Drug StudyAllyne GavinoNo ratings yet
- Burn - Concept MapDocument1 pageBurn - Concept MapAaron RafaelNo ratings yet
- Drug StudyDocument2 pagesDrug StudyCen Janber CabrillosNo ratings yet
- As Pi LetDocument7 pagesAs Pi Letianecunar100% (1)
- Aspirin Drug SummDocument2 pagesAspirin Drug SummWarren0% (1)
- Drug Study. GeamhDocument5 pagesDrug Study. GeamhMacky RobentaNo ratings yet
- Drug Study - MorphineDocument3 pagesDrug Study - MorphineKian HerreraNo ratings yet
- EsmololDocument2 pagesEsmololtherock316_995149No ratings yet
- Nitroglycerin Drug StudyDocument2 pagesNitroglycerin Drug StudyBeatrizz P GellaNo ratings yet
- Generic Name: Brand Name:: ClassificationsDocument2 pagesGeneric Name: Brand Name:: ClassificationsbillyktoubattsNo ratings yet
- Doxorubicin Dosage, Uses, Side Effects and Nursing CareDocument4 pagesDoxorubicin Dosage, Uses, Side Effects and Nursing CareMaryjoy Gabriellee De La CruzNo ratings yet
- Tramadol and Ciprofloxacin: Key Information for NursesDocument2 pagesTramadol and Ciprofloxacin: Key Information for NursesatchiekNo ratings yet
- Drug Study (Acetaminophen)Document1 pageDrug Study (Acetaminophen)Kian HerreraNo ratings yet
- CombiventDocument1 pageCombiventDherick Rosas0% (1)
- Losartan Drug StudyDocument2 pagesLosartan Drug StudyXerxes DejitoNo ratings yet
- Wesleyan: College of Nursing and Allied Medical SciencesDocument2 pagesWesleyan: College of Nursing and Allied Medical SciencesShane Aileen AngelesNo ratings yet
- Drug Study - OB WardDocument8 pagesDrug Study - OB WardCheska YsabelleNo ratings yet
- Drug AnalysisDocument3 pagesDrug AnalysisAnn Aquino100% (1)
- Drug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesDocument1 pageDrug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesSheryhan Tahir BayleNo ratings yet
- Drug AnalysisDocument18 pagesDrug AnalysisArt Christian RamosNo ratings yet
- Drug Study - Acetaminophen, ParacetamolDocument1 pageDrug Study - Acetaminophen, ParacetamolmikErlh100% (2)
- Drug StudyDocument4 pagesDrug StudyXio PauNo ratings yet
- Drug Study QIDocument8 pagesDrug Study QImaeDonitaNo ratings yet
- Aerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatec Rinovagos, Atrovent, Atrovent HFADocument3 pagesAerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatec Rinovagos, Atrovent, Atrovent HFAGwyn RosalesNo ratings yet
- Aerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatecrinovagos, Atrovent, Atrovent HfaDocument4 pagesAerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatecrinovagos, Atrovent, Atrovent HfaGwyn RosalesNo ratings yet
- Drug Study - Salbutamol + IpratropiumDocument4 pagesDrug Study - Salbutamol + IpratropiumJade Mikaela0% (1)
- Name of DrugDocument5 pagesName of DrugJoann BeriñoNo ratings yet
- Vancomycin (Hospital Formulary) - LexicompDocument1 pageVancomycin (Hospital Formulary) - Lexicompsalmanul farisNo ratings yet
- Ipratroprium Drug CardDocument3 pagesIpratroprium Drug CardXiaoDuckyNo ratings yet
- PhenobarbitalDocument6 pagesPhenobarbitalGwyn RosalesNo ratings yet
- NimodipineDocument5 pagesNimodipineGwyn Rosales100% (1)
- IronDocument3 pagesIronGwyn RosalesNo ratings yet
- Nursing responsibilities for CotrimoxazoleDocument5 pagesNursing responsibilities for CotrimoxazoleGwyn RosalesNo ratings yet
- LevetiracetamDocument4 pagesLevetiracetamGwyn RosalesNo ratings yet
- IntralipidDocument3 pagesIntralipidGwyn RosalesNo ratings yet
- DiphenhydramineDocument3 pagesDiphenhydramineGwyn RosalesNo ratings yet
- ESOMEPRAZOLEDocument6 pagesESOMEPRAZOLEGwyn RosalesNo ratings yet
- Combivent Nursing ResponsibilitiesDocument2 pagesCombivent Nursing ResponsibilitiesGwyn RosalesNo ratings yet
- CeftriaDocument5 pagesCeftriaGwyn RosalesNo ratings yet
- CebUN Drug Study for HypothyroidismDocument4 pagesCebUN Drug Study for HypothyroidismGwyn RosalesNo ratings yet
- GliclazideDocument5 pagesGliclazideGwyn RosalesNo ratings yet
- CEFUROXIMEDocument3 pagesCEFUROXIMEGwyn RosalesNo ratings yet
- EnalaprilDocument4 pagesEnalaprilGwyn RosalesNo ratings yet
- DexamethasoneDocument3 pagesDexamethasoneGwyn RosalesNo ratings yet
- ColistinDocument2 pagesColistinGwyn RosalesNo ratings yet
- DiazepamDocument3 pagesDiazepamGwyn RosalesNo ratings yet
- CefoxitinDocument3 pagesCefoxitinGwyn RosalesNo ratings yet
- CiticolineDocument3 pagesCiticolineGwyn RosalesNo ratings yet
- Per System PreferablyDocument2 pagesPer System PreferablyGwyn RosalesNo ratings yet
- Tetanus ToxoidDocument3 pagesTetanus ToxoidGwyn Rosales100% (1)
- General Indications: Body As A Whole: Allergy,: Therapeutic EffectDocument3 pagesGeneral Indications: Body As A Whole: Allergy,: Therapeutic EffectGwyn RosalesNo ratings yet
- (Per System Preferably) : AntihypertensiveDocument4 pages(Per System Preferably) : AntihypertensiveGwyn RosalesNo ratings yet
- Per System PreferablyDocument3 pagesPer System PreferablyGwyn RosalesNo ratings yet
- CapecitabineDocument2 pagesCapecitabineGwyn RosalesNo ratings yet
- CaptoprilDocument3 pagesCaptoprilGwyn RosalesNo ratings yet
- Amikacin Sulfate Nursing ResponsibilitiesDocument2 pagesAmikacin Sulfate Nursing ResponsibilitiesGwyn Rosales100% (2)
- Per System PreferablyDocument4 pagesPer System PreferablyGwyn RosalesNo ratings yet
- Amlodipine Reduces Systolic, Diastolic, and Mean Arterial Blood Pressure. It Also Decreases Pain Due To AnginaDocument2 pagesAmlodipine Reduces Systolic, Diastolic, and Mean Arterial Blood Pressure. It Also Decreases Pain Due To AnginaGwyn RosalesNo ratings yet
- Per System PreferablyDocument3 pagesPer System PreferablyGwyn RosalesNo ratings yet
- Surat Kecil Untuk TuhanDocument9 pagesSurat Kecil Untuk TuhanAsgarPurnamaNo ratings yet
- K2N Final Internship ReportDocument55 pagesK2N Final Internship ReportAceZeta0% (1)
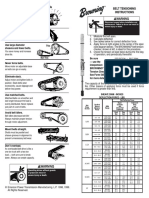
- Browning Belt Tension GaugeDocument2 pagesBrowning Belt Tension GaugeJasperken2xNo ratings yet
- November 2010 (v1) QP - Paper 3 CIE Biology A-Level PDFDocument12 pagesNovember 2010 (v1) QP - Paper 3 CIE Biology A-Level PDFWiji NingNo ratings yet
- IRIScan Book Executive 3 PDFDocument86 pagesIRIScan Book Executive 3 PDFssamplingNo ratings yet
- ES vs SIGINT: Understanding the DifferencesDocument9 pagesES vs SIGINT: Understanding the DifferencesYasir ShigileeniNo ratings yet
- Revision 2 Pages Grammar Drills 106078Document3 pagesRevision 2 Pages Grammar Drills 106078Ligia Dragomir100% (1)
- Analog Layout Design (Industrial Training)Document10 pagesAnalog Layout Design (Industrial Training)Shivaksh SharmaNo ratings yet
- #10 VHB SGT-APT Design SummaryDocument2 pages#10 VHB SGT-APT Design SummarySenthil KumarNo ratings yet
- Labcelldivision ErikagutierrezDocument10 pagesLabcelldivision Erikagutierrezapi-336047220No ratings yet
- DesignDocument2 pagesDesignAmr AbdalhNo ratings yet
- Biomass and Bioenergy: Z.N. Akhlisah, R. Yunus, Z.Z. Abidin, B.Y. Lim, D. KaniaDocument20 pagesBiomass and Bioenergy: Z.N. Akhlisah, R. Yunus, Z.Z. Abidin, B.Y. Lim, D. KaniaPutri sinagaNo ratings yet
- Roland Berger Hot Trends InconstructionDocument24 pagesRoland Berger Hot Trends InconstructionJavier ContrerasNo ratings yet
- Aula 4 - Wooten - Organizational FieldsDocument28 pagesAula 4 - Wooten - Organizational FieldsferreiraccarolinaNo ratings yet
- Mechanical Design of Turine EginesDocument51 pagesMechanical Design of Turine EginessriniNo ratings yet
- 60d068822a861e19f4179ec9 - 11. Consensus - Local Cerberus - CompressedDocument1 page60d068822a861e19f4179ec9 - 11. Consensus - Local Cerberus - Compressedhombre pocilgaNo ratings yet
- Foundation of EducationDocument31 pagesFoundation of EducationM T Ząřřąř100% (1)
- Figure of SpeechDocument27 pagesFigure of SpeechSabel Ross CaliliwNo ratings yet
- Line Pack Presentation - Dec 2018Document7 pagesLine Pack Presentation - Dec 2018Goran JakupovićNo ratings yet
- Flange Insulation Sets: Technical SpecificationDocument6 pagesFlange Insulation Sets: Technical SpecificationNor Azlan AwangNo ratings yet
- Determine PH by PH Indicator and Universal IndicatorDocument3 pagesDetermine PH by PH Indicator and Universal IndicatorhaleelNo ratings yet
- Ceiling Fans Sensa Series: F Yuragi Function (Natural Breeze)Document1 pageCeiling Fans Sensa Series: F Yuragi Function (Natural Breeze)TYNo ratings yet
- Make A Selection: Choose An Alloy and Correlating Casting ProcessDocument5 pagesMake A Selection: Choose An Alloy and Correlating Casting ProcessSarath ChandraNo ratings yet
- Rate Constant Determination 2Document8 pagesRate Constant Determination 2Divya UpadhyayNo ratings yet
- Blackmer Pump Parts ListDocument2 pagesBlackmer Pump Parts ListFelipe Ignacio PaillavilNo ratings yet
- Rate Analysis-Norms 1Document10 pagesRate Analysis-Norms 1yamanta_rajNo ratings yet
- Fundamentals of Wind EnergyDocument24 pagesFundamentals of Wind EnergyMas3odNo ratings yet
- SilverDocument16 pagesSilversharma_shruti0% (1)
- RTWP OptimisationHanFeedbackDocument31 pagesRTWP OptimisationHanFeedbackSeth Mawuli Dedzoe100% (1)
- AstigmatismDocument1 pageAstigmatismAmmellya PutriNo ratings yet