You might also like
- Edtpa Lesson Plan 1-4Document16 pagesEdtpa Lesson Plan 1-4api-457218566100% (5)
- Chapter 1 Thinking Critically With Psychological Science, Myers 8e PsychologyDocument26 pagesChapter 1 Thinking Critically With Psychological Science, Myers 8e Psychologymrchubs100% (7)
- Unethical Practices in Conducting Research: Factors To Consider in Selecting A Research ProblemDocument7 pagesUnethical Practices in Conducting Research: Factors To Consider in Selecting A Research ProblemJimin ParkNo ratings yet
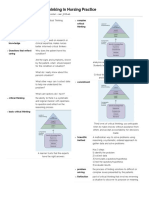
- Critical Thinking in Nursing PracticeDocument3 pagesCritical Thinking in Nursing PracticeAutumn GarofolaNo ratings yet
- Act1 3isDocument1 pageAct1 3isG-VALDEZ, SHELAHNo ratings yet
- Funda Lec MidtermsDocument13 pagesFunda Lec MidtermsCharisse CaydanNo ratings yet
- (PS 109) ResearchDocument4 pages(PS 109) ResearchKaryfe Von OrtezaNo ratings yet
- ResearchDocument1 pageResearchnkcsantosNo ratings yet
- MidtermsDocument5 pagesMidtermsJianne CaloNo ratings yet
- Philosophy of Accounting ThoughtDocument9 pagesPhilosophy of Accounting ThoughtTheGilmoreBuddiesNo ratings yet
- Conceptualization of Research: What? Why? How?Document68 pagesConceptualization of Research: What? Why? How?pragyasimsNo ratings yet
- 1 Funda Lec Critical Thinking and Nursing DiagnosisDocument5 pages1 Funda Lec Critical Thinking and Nursing DiagnosisAudrey Beatrice ReyesNo ratings yet
- Practical Research ReviewerDocument4 pagesPractical Research ReviewerCarolyn AlvarezNo ratings yet
- Lesson 1: The Nature of Research and The Research Process: Read To LearnDocument4 pagesLesson 1: The Nature of Research and The Research Process: Read To LearnIvan Karl LobatonNo ratings yet
- Nursing ProcessDocument4 pagesNursing ProcessCrazy StrangerNo ratings yet
- 02 Research MethodsDocument9 pages02 Research MethodsTunahan OğuzNo ratings yet
- Reviewer MidtermsDocument12 pagesReviewer MidtermsyyyyepyepNo ratings yet
- Revision of Ct and Sample Mid Course Test 30-9-2018 Đã Chuyển ĐổiDocument14 pagesRevision of Ct and Sample Mid Course Test 30-9-2018 Đã Chuyển Đổily luuNo ratings yet
- Field Methods - Unit 1Document51 pagesField Methods - Unit 1VK VillNo ratings yet
- Nursing Research Course Packet 2Document7 pagesNursing Research Course Packet 2keiiiNo ratings yet
- Chapter 1Document15 pagesChapter 1CAPINIANES MARY ABIGAILNo ratings yet
- Research ApproachDocument5 pagesResearch Approachgdayanand4uNo ratings yet
- Critical ThinkingDocument5 pagesCritical ThinkingEugelyn BondocNo ratings yet
- Research ReviewerDocument3 pagesResearch ReviewerJM GNo ratings yet
- Designing Naturalistic InquiryDocument19 pagesDesigning Naturalistic InquiryEko SaputraNo ratings yet
- PasadoDocument9 pagesPasadoalanamaya901No ratings yet
- PR1 11 Q1 Week 1Document22 pagesPR1 11 Q1 Week 1Lex Aine June D. TaborNo ratings yet
- Berpikir KritisDocument19 pagesBerpikir KritisZain Karim100% (1)
- Practical Research 1 ReviewerDocument13 pagesPractical Research 1 Reviewerjamifatie21No ratings yet
- Chapter 2Document19 pagesChapter 2Ashley SunNo ratings yet
- Scientific ThinkingDocument6 pagesScientific ThinkingremyramblesNo ratings yet
- Prac ResDocument5 pagesPrac Rescuasayprincessnicole4No ratings yet
- 2nd-Semester-Midterm-Reviewer 3Document48 pages2nd-Semester-Midterm-Reviewer 3Justin BorjaNo ratings yet
- LLT - Chapter 13 - Presentation Group 1&2Document11 pagesLLT - Chapter 13 - Presentation Group 1&2Greacia MayoNo ratings yet
- Chapter 3 Qualitative Research NotesDocument4 pagesChapter 3 Qualitative Research NotesCheryl OrtizNo ratings yet
- PR 1 ReviewerDocument7 pagesPR 1 ReviewerJAMES GAMERNo ratings yet
- Research in Daily Life 1 - ReviewerDocument6 pagesResearch in Daily Life 1 - Reviewerdivinegrace.cruz.mnlNo ratings yet
- Evidence-Based Practice and Research in NursingDocument4 pagesEvidence-Based Practice and Research in NursingCrazy StrangerNo ratings yet
- Activity 2: Quantitative Research Qualitative ResearchDocument1 pageActivity 2: Quantitative Research Qualitative ResearchLia SyNo ratings yet
- How Do Physical Therapists Make Clinical Decisions?: Dr. Haider Darain PHD, MSC, BSPTDocument16 pagesHow Do Physical Therapists Make Clinical Decisions?: Dr. Haider Darain PHD, MSC, BSPTAliza maryNo ratings yet
- PR ReviewerDocument3 pagesPR ReviewerAiko NanaseNo ratings yet
- Definition, Problem Identification ObjectivesDocument6 pagesDefinition, Problem Identification ObjectivesKunal DasNo ratings yet
- Bus 500Document13 pagesBus 500hira syedNo ratings yet
- Research Methodology QuestionsDocument4 pagesResearch Methodology QuestionsMohamed HussienNo ratings yet
- Major Importance: Importance of Nursing Theory inDocument3 pagesMajor Importance: Importance of Nursing Theory inXyrielle GarciaNo ratings yet
- Practical Research 2 Humss 4Document13 pagesPractical Research 2 Humss 4Oliver CarsolemNo ratings yet
- Week 2 - Phases & Processes of Psychotherapy and Micro-Counselling SkillsDocument19 pagesWeek 2 - Phases & Processes of Psychotherapy and Micro-Counselling SkillsPhuwadej VorasowharidNo ratings yet
- Adapting Scott and Bruce's General Decision-Making Style Inventory To Patient Decision Making in Provider ChoiceDocument8 pagesAdapting Scott and Bruce's General Decision-Making Style Inventory To Patient Decision Making in Provider ChoiceAntonuonNo ratings yet
- B5RESMETDocument21 pagesB5RESMETSandy TafallaNo ratings yet
- Research in Daily Life 2Document11 pagesResearch in Daily Life 2Krizel Sadang100% (1)
- Experimental Psychology Chapter 1 Experimental Psychology and The Scientific MethodDocument3 pagesExperimental Psychology Chapter 1 Experimental Psychology and The Scientific MethodBasada, Doie Jake B.No ratings yet
- Hypothesis - Concept and TypesDocument38 pagesHypothesis - Concept and TypesAstha PooniaNo ratings yet
- RM-2 ScyDocument58 pagesRM-2 ScyHabtamu GaromaNo ratings yet
- Nurses Role in Health Assessment and Nursing ProcessDocument9 pagesNurses Role in Health Assessment and Nursing ProcessJasmine MayeNo ratings yet
- Rise, Reframe, Reflect: A Guide to Cultivating Powerful Thinking HabitsFrom EverandRise, Reframe, Reflect: A Guide to Cultivating Powerful Thinking HabitsNo ratings yet
- Methods and Evaluation in Clinical and Counseling Psychology: Pergamon General Psychology SeriesFrom EverandMethods and Evaluation in Clinical and Counseling Psychology: Pergamon General Psychology SeriesRating: 4 out of 5 stars4/5 (1)
- Critical Minds, Creative Solutions: Nurturing Analytical Thinking and Innovation.From EverandCritical Minds, Creative Solutions: Nurturing Analytical Thinking and Innovation.No ratings yet
- Critical Thinking Revolutionized: The New Science Behind Creative Problem Solving, Evaluating Information and Making Right DecisionsFrom EverandCritical Thinking Revolutionized: The New Science Behind Creative Problem Solving, Evaluating Information and Making Right DecisionsNo ratings yet
- Human Judgment and Decision Processes in Applied SettingsFrom EverandHuman Judgment and Decision Processes in Applied SettingsMartin F. KaplanNo ratings yet
- The Effects of Music On Short-Term and Long-Term MemoryDocument25 pagesThe Effects of Music On Short-Term and Long-Term MemoryLustre GlarNo ratings yet
- Science and Engineering: Background/IntroductionDocument8 pagesScience and Engineering: Background/IntroductionLustre GlarNo ratings yet
- Basketball Hand SignalsDocument17 pagesBasketball Hand SignalsLustre GlarNo ratings yet
- Basketball OfficiatingDocument12 pagesBasketball OfficiatingLustre GlarNo ratings yet
- 1 Sigmund Freud-PsychoanalysisDocument6 pages1 Sigmund Freud-PsychoanalysisLustre GlarNo ratings yet
- 5 Melanie Klein-Object Relations TheoryDocument4 pages5 Melanie Klein-Object Relations TheoryLustre GlarNo ratings yet
- 4 Carl Jung - Analytical PsychologyDocument4 pages4 Carl Jung - Analytical PsychologyLustre GlarNo ratings yet
- 2 Cognitive NeuroscienceDocument33 pages2 Cognitive NeuroscienceLustre GlarNo ratings yet
- Perception: Test Yourself 3.2Document33 pagesPerception: Test Yourself 3.2Lustre GlarNo ratings yet
- Sleeping For Exam Success - TranscriptDocument2 pagesSleeping For Exam Success - TranscriptAmir AslanNo ratings yet
- Elective PPT Product DesignDocument9 pagesElective PPT Product Design10Aboli MahajanNo ratings yet
- Motivasi Dalam Konteks Human Relations: Mudzhira Nur AmrullahDocument12 pagesMotivasi Dalam Konteks Human Relations: Mudzhira Nur AmrullahEfras AjiNo ratings yet
- Madurai 2Document4 pagesMadurai 2Suresh Lakshmi NarasimhanNo ratings yet
- Text To Self Editedenglish 9 Quarter 2 Module 1Document8 pagesText To Self Editedenglish 9 Quarter 2 Module 1Bronil, John Angelo J.No ratings yet
- Laura Mendieta PTP 1Document4 pagesLaura Mendieta PTP 1api-543309118No ratings yet
- Media and Information Literacy - Q4 - Week 11Document6 pagesMedia and Information Literacy - Q4 - Week 11Angelo MartinezNo ratings yet
- Discourse Analysis and Pragmatics Their Scope and RelationDocument13 pagesDiscourse Analysis and Pragmatics Their Scope and RelationNguyễn Hoàng Minh AnhNo ratings yet
- Educational PsychologyDocument204 pagesEducational PsychologyAthumani Shaaban IssaNo ratings yet
- Human Resource Management SESSION 5-6Document26 pagesHuman Resource Management SESSION 5-6Neeraj shekharNo ratings yet
- Defining Bilingualism PDFDocument8 pagesDefining Bilingualism PDFKhenjeza PornelaNo ratings yet
- SValdilles Exam 1 AutismDocument3 pagesSValdilles Exam 1 AutismSunshine Corliss ValdillesNo ratings yet
- E-Journal Metrouniv Ac IdDocument10 pagesE-Journal Metrouniv Ac IdmilzamamelNo ratings yet
- Human Visual PerceptionDocument14 pagesHuman Visual PerceptionMukunda Chaitanya AkkaliNo ratings yet
- Bsed 1 - Understanding The Self Week 3-4Document2 pagesBsed 1 - Understanding The Self Week 3-4Laarni ToleteNo ratings yet
- Properties of LightDocument2 pagesProperties of Lightapi-619073913No ratings yet
- MET RatingScale SpeakingDocument1 pageMET RatingScale SpeakingLancer2kSNo ratings yet
- Importance of Graphic Organizers For PhysicsDocument3 pagesImportance of Graphic Organizers For PhysicsHammad Siraj AhmedNo ratings yet
- 3rd Grading-Handling Guest ComplaintsDocument2 pages3rd Grading-Handling Guest ComplaintsRey J I. Gonzales100% (2)
- DLP Health 4Document11 pagesDLP Health 4Met Xii100% (2)
- Problems and Factors Affecting Listening & SpeakingDocument21 pagesProblems and Factors Affecting Listening & SpeakingHaressh BhavaniiNo ratings yet
- Enbrighten Scoring Rubric - Five ScoresDocument1 pageEnbrighten Scoring Rubric - Five Scoresapi-256301743No ratings yet
- Quarterly Curriculum Guide - Mother Tongue (MT) : Content Standard - 1 QuarterDocument30 pagesQuarterly Curriculum Guide - Mother Tongue (MT) : Content Standard - 1 QuarterAices Jasmin Melgar BongaoNo ratings yet
- Benefits of Multiple IntelligencesDocument3 pagesBenefits of Multiple IntelligencesAleen SalehNo ratings yet
- B. Culture and Arts Education in The Philippines (Theories, History, and Legal Basis, The Role of Art Education in The 21 Century)Document6 pagesB. Culture and Arts Education in The Philippines (Theories, History, and Legal Basis, The Role of Art Education in The 21 Century)Aron GeromoNo ratings yet
- Learning Disabilities PowerPointDocument21 pagesLearning Disabilities PowerPointPriyaNo ratings yet
- Oral Communication Week 1Document22 pagesOral Communication Week 1Mhagz MaggieNo ratings yet
- Theories of Language Acquisition: By: Joannacel AbrinaDocument20 pagesTheories of Language Acquisition: By: Joannacel AbrinaAlbert Joe Abrina100% (1)
- 5th Group DesuggestopediaDocument8 pages5th Group DesuggestopediaAfg-Ghynhaalfiyah Chyllowend Arisyhaa KeiinhaLynchNo ratings yet