You might also like
- Obstetric - OB Ultrasound Made Easy - Step-By-Step Guide - POCUS 101Document42 pagesObstetric - OB Ultrasound Made Easy - Step-By-Step Guide - POCUS 101skype72214100% (1)
- Nbme 30 2021 ADocument200 pagesNbme 30 2021 AUsama Bilal100% (3)
- Health: Quarter 1-Module 6Document25 pagesHealth: Quarter 1-Module 6Niko Igie Albino Pujeda0% (1)
- March 2015 Recalls Mrcog p2 DR Hamada Aboromuh PDFDocument76 pagesMarch 2015 Recalls Mrcog p2 DR Hamada Aboromuh PDFuzairNo ratings yet
- Imaging in Genitourinary System - 17 Agustus 2013 - by Robby HermawanDocument80 pagesImaging in Genitourinary System - 17 Agustus 2013 - by Robby HermawanFitria Dewi LestariNo ratings yet
- C+F-Urinary Incontinence in Dogs and Cats - Part II. Diagnosis and ManagementDocument11 pagesC+F-Urinary Incontinence in Dogs and Cats - Part II. Diagnosis and Managementtaner_soysuren100% (2)
- Genitourinary SystemDocument8 pagesGenitourinary Systemsarguss14100% (1)
- Carcinoma of The CervixDocument5 pagesCarcinoma of The CervixMuhammadR1100% (1)
- Concept Map On AppendicitisDocument6 pagesConcept Map On Appendicitisitalisayan_rondario80% (5)
- Interstitial CystitisDocument9 pagesInterstitial CystitisKousik Amancharla100% (3)
- Pre Conception Care - Who GuidelinesDocument26 pagesPre Conception Care - Who GuidelinesrekhamolNo ratings yet
- Family Planning Client Assessment FormDocument3 pagesFamily Planning Client Assessment FormGeline Joy D. Samillano100% (3)
- Nursing Responsibilities Adverse Effect Indication / Contraindication Mechanism of Action Drug Name IndicationDocument1 pageNursing Responsibilities Adverse Effect Indication / Contraindication Mechanism of Action Drug Name IndicationOmar Izzo100% (1)
- Husband's House-Novel by Moyosore TeniolaDocument157 pagesHusband's House-Novel by Moyosore TeniolaEny100% (5)
- Neurogenic BladderDocument11 pagesNeurogenic BladderRoy LiemNo ratings yet
- Urinery IncontinsetenceDocument1 pageUrinery IncontinsetenceLanaAmerieNo ratings yet
- UrinaryDocument19 pagesUrinaryfiel borataNo ratings yet
- Nursing Care Plan: RationaleDocument5 pagesNursing Care Plan: Rationalerona-chanNo ratings yet
- Benign Prostatic HyperplasiaDocument5 pagesBenign Prostatic Hyperplasiatabangin_hilario100% (1)
- Evaluation of The Incontinent Woman: Yeditepe University, Medical Faculty Dept of Ob&GynDocument47 pagesEvaluation of The Incontinent Woman: Yeditepe University, Medical Faculty Dept of Ob&GynAdnan WalidNo ratings yet
- MS 2Document8 pagesMS 2Vincent AmitNo ratings yet
- MATERI SESI 4.1 - MAR DR - HeryDocument9 pagesMATERI SESI 4.1 - MAR DR - HerydewiswahyuNo ratings yet
- UrinaryDocument3 pagesUrinaryAlyssa Jade GolezNo ratings yet
- Insignis Pedia Red Flags of Renal DiseasesDocument4 pagesInsignis Pedia Red Flags of Renal DiseasesBinod Kumar SahNo ratings yet
- Kub IvpDocument46 pagesKub IvpBryJos tiongsonNo ratings yet
- 3 Urinary Incontinence in WomenDocument4 pages3 Urinary Incontinence in WomenDanilo Pereira Dos SantosNo ratings yet
- Inkontinensia Urin: Dr. Adhi Permana, SPPDDocument35 pagesInkontinensia Urin: Dr. Adhi Permana, SPPDtutor tujuhNo ratings yet
- Symptomatology of GUT DisordersDocument75 pagesSymptomatology of GUT DisordersMaraJoRNNo ratings yet
- Inkontinensia Urin: Dr. Adhi Permana, SPPDDocument35 pagesInkontinensia Urin: Dr. Adhi Permana, SPPDTiara KhairinaNo ratings yet
- Imaging of The Genitourinary Tract: Mashuri, DR.,SP - Rad.,M.KesDocument90 pagesImaging of The Genitourinary Tract: Mashuri, DR.,SP - Rad.,M.KesmirzasullivanNo ratings yet
- UrinaryDocument3 pagesUrinaryAlyssa Jade GolezNo ratings yet
- Appendix Anatomy: SURGERY 2 - G.I. ModuleDocument2 pagesAppendix Anatomy: SURGERY 2 - G.I. ModuleFrances Isabella OlasimanNo ratings yet
- Chap 23Document25 pagesChap 23Ghazian AdliNo ratings yet
- Chapter 6 - Genitourinary SystemDocument41 pagesChapter 6 - Genitourinary Systemsnowlover boyNo ratings yet
- Inkontinensia UrinDocument24 pagesInkontinensia UrinloyaNo ratings yet
- WK5 - Urinary Catheterization (Dash 10)Document3 pagesWK5 - Urinary Catheterization (Dash 10)kristelaaa guevarraNo ratings yet
- Managing LUTS BPH For Patients at Risk of Progression - DR RickyDocument37 pagesManaging LUTS BPH For Patients at Risk of Progression - DR RickyafifberlianNo ratings yet
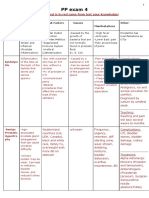
- PP Exam 4: Everything That Is in Red Came From Test Your Knowledge!Document15 pagesPP Exam 4: Everything That Is in Red Came From Test Your Knowledge!netanya DoanNo ratings yet
- 3 Obat Sedasi Dan Analgesia-Prof Munar - LubisDocument93 pages3 Obat Sedasi Dan Analgesia-Prof Munar - LubisFahmi NurNo ratings yet
- Evidence Statement Anal Incontinence Flowchart PDFDocument2 pagesEvidence Statement Anal Incontinence Flowchart PDFsilkofosNo ratings yet
- KNGF Evidence Statement: Anal IncontinenceDocument2 pagesKNGF Evidence Statement: Anal IncontinencesilkofosNo ratings yet
- Inkontinensia UrinDocument27 pagesInkontinensia Urinyuni100% (1)
- HARLE FinalsDocument15 pagesHARLE Finalsangelapadilla0893No ratings yet
- Miss Salam PresentationDocument3 pagesMiss Salam PresentationyuddNo ratings yet
- MS 2Document9 pagesMS 2Vincent AmitNo ratings yet
- MENISCODocument26 pagesMENISCOSarah SiraitNo ratings yet
- Urologist.: Stress IncontinenceDocument2 pagesUrologist.: Stress IncontinenceJ MNo ratings yet
- Creog Urogyn ReviewDocument97 pagesCreog Urogyn ReviewAlexandriah AlasNo ratings yet
- 990812 EUS教學 (4) 重點式急診泌尿系統超音波之應用Document77 pages990812 EUS教學 (4) 重點式急診泌尿系統超音波之應用juice119100% (2)
- Urinary EliminationDocument7 pagesUrinary EliminationwowsamanthaNo ratings yet
- Fundamentals of Nursing RLE FinalsDocument37 pagesFundamentals of Nursing RLE FinalsSofia Denise JoseNo ratings yet
- NCM 30 C. 46Document9 pagesNCM 30 C. 46Marlo FredNo ratings yet
- Male and Female Radiographic ProceduresDocument5 pagesMale and Female Radiographic ProceduresKaye A. JardinicoNo ratings yet
- Urological Symptomatology in Patients With Reflex Sympathetic DystrophyDocument8 pagesUrological Symptomatology in Patients With Reflex Sympathetic DystrophyMihaela LitovcencoNo ratings yet
- Introduction To UrinalysisDocument8 pagesIntroduction To UrinalysisKyle PicocNo ratings yet
- Basics of Urology 1Document29 pagesBasics of Urology 1gozali189 biringNo ratings yet
- Urological Emergencies: Julian ManderDocument43 pagesUrological Emergencies: Julian ManderDara MirandaNo ratings yet
- Male Reproductive DisordersDocument8 pagesMale Reproductive DisordersElaine Francisse TampusNo ratings yet
- Bladder Funtion MBBS 2009Document24 pagesBladder Funtion MBBS 2009Deshan AdikariNo ratings yet
- MEDSURG Urinary SystemDocument7 pagesMEDSURG Urinary SystemQV MangubatNo ratings yet
- Isk BSKDocument5 pagesIsk BSKAndy F MonroeNo ratings yet
- Patho SlidesDocument26 pagesPatho Slidesapi-725203846No ratings yet
- Imaging of The Genitourinary TractDocument86 pagesImaging of The Genitourinary TractNor AinaNo ratings yet
- CKD History TakingDocument2 pagesCKD History TakingNadia Salwani80% (5)
- Timbul Sakulasi Atau DivertikelDocument2 pagesTimbul Sakulasi Atau DivertikelRendi PotlotNo ratings yet
- Renal System (Output)Document30 pagesRenal System (Output)Tiffy SuarezNo ratings yet
- 296 - Renal Pathology) Respiratory AcidosisDocument4 pages296 - Renal Pathology) Respiratory AcidosisMuhammadR1No ratings yet
- Notice For Dip PEC (SA) - FS 2023 13 1 2024Document1 pageNotice For Dip PEC (SA) - FS 2023 13 1 2024MuhammadR1No ratings yet
- The Concept of Syed Muhammad Naquib Al-Attas On deDocument21 pagesThe Concept of Syed Muhammad Naquib Al-Attas On deMuhammadR1No ratings yet
- FC Rad Diag (SA) Part I Past Papers - 2018 2nd Semester 31 8 2023Document2 pagesFC Rad Diag (SA) Part I Past Papers - 2018 2nd Semester 31 8 2023MuhammadR1No ratings yet
- EndometriosisDocument8 pagesEndometriosisMuhammadR1No ratings yet
- InfertilityDocument10 pagesInfertilityMuhammadR1No ratings yet
- Hyperemesis GravidarumDocument16 pagesHyperemesis Gravidarumchithra vijay100% (1)
- Conquering InfertilityDocument48 pagesConquering InfertilityO'David KreationsNo ratings yet
- Medical English Vocab.Document21 pagesMedical English Vocab.Özgür ÇınarNo ratings yet
- Class 12 Investigatory Project....Document8 pagesClass 12 Investigatory Project....shivshankardahayat80No ratings yet
- Poonam Sharma V Union of IndiaDocument14 pagesPoonam Sharma V Union of Indiakritik roshan RVNo ratings yet
- SHARK - Circulation, Respiration and Reprodutive System: Dr.M.DeivanayakiDocument10 pagesSHARK - Circulation, Respiration and Reprodutive System: Dr.M.DeivanayakiNavin KumarNo ratings yet
- Child Health Services-1Document44 pagesChild Health Services-1francisNo ratings yet
- DRUG-STUDY-OB Ward BLHDocument1 pageDRUG-STUDY-OB Ward BLHDianne UlandayNo ratings yet
- PC-1 IRMNCH and NP Punjab 2015-17Document120 pagesPC-1 IRMNCH and NP Punjab 2015-17Ejaz AhmadNo ratings yet
- Assefa MitikuDocument70 pagesAssefa Mitikufiraol mokonnenNo ratings yet
- Hypoglycemia in Exclusively Breastfed High-Risk Neonates - A Hospital-Based StudyDocument7 pagesHypoglycemia in Exclusively Breastfed High-Risk Neonates - A Hospital-Based StudyNeta Aza MaineztNo ratings yet
- MANUSKRIP Luluk Eka MeylawatiDocument7 pagesMANUSKRIP Luluk Eka MeylawatiYelpita DewiNo ratings yet
- Lesson-24-145 - KEYDocument11 pagesLesson-24-145 - KEYTrang YenNo ratings yet
- Embryo TransferDocument21 pagesEmbryo TransferMARCO ANTONIO CABRERA PASCACIONo ratings yet
- Nursing Care Related To Psychological and Physiological Changes of PregnancyDocument180 pagesNursing Care Related To Psychological and Physiological Changes of PregnancyJohanine VillasantiagoNo ratings yet
- IGCSE Biology - TOPIC 14 - Endocrine System & Homeostasis SUMMARY NOTESDocument8 pagesIGCSE Biology - TOPIC 14 - Endocrine System & Homeostasis SUMMARY NOTESpeggyyu12345No ratings yet
- The Promise of Greatness: Women and PowerDocument4 pagesThe Promise of Greatness: Women and PowerGriffin GonzalesNo ratings yet
- Neonatal HypothermiaDocument8 pagesNeonatal Hypothermiamia liaNo ratings yet
- Test Bank For Adolescence 9th Edition SteinbergDocument37 pagesTest Bank For Adolescence 9th Edition Steinbergryanngossman17912558100% (14)
- CHN Epidemiology and Vital StatisticsDocument33 pagesCHN Epidemiology and Vital StatisticsRolando FaustoNo ratings yet
- Sample ChapterDocument10 pagesSample ChapterTofik MohammedNo ratings yet
- P D F F M: OST Octoral Ellowship IN Etal EdicineDocument2 pagesP D F F M: OST Octoral Ellowship IN Etal Edicinegowthamsince89No ratings yet
- PRULady-Brochure New 2023Document12 pagesPRULady-Brochure New 2023佳昇.No ratings yet