Professional Documents
Culture Documents
A Community-Engaged Project Discovering The Sexuality Questions of Adults With Intellectual and Developmental Disabilities
Uploaded by
Asish DasOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
A Community-Engaged Project Discovering The Sexuality Questions of Adults With Intellectual and Developmental Disabilities
Uploaded by
Asish DasCopyright:
Available Formats
See discussions, stats, and author profiles for this publication at: https://www.researchgate.
net/publication/349610944
A Community-Engaged Project Discovering the Sexuality Questions of Adults
With Intellectual and Developmental Disabilities
Article in Inclusion · March 2021
DOI: 10.1352/2326-6988-9.1.2
CITATIONS READS
0 181
3 authors:
Rebecca Kammes Rhonda S. Black
Michigan State University University of Hawai'i System
16 PUBLICATIONS 179 CITATIONS 54 PUBLICATIONS 1,582 CITATIONS
SEE PROFILE SEE PROFILE
Trisha Easley
Michigan State University
3 PUBLICATIONS 10 CITATIONS
SEE PROFILE
Some of the authors of this publication are also working on these related projects:
Disability and Gender-based Violence View project
Self-determination for Culturally and Linguistically Diverse Students with Disabilities View project
All content following this page was uploaded by Rhonda S. Black on 02 March 2021.
The user has requested enhancement of the downloaded file.
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
A Community-Engaged Project Discovering the Sexuality
Questions of Adults With Intellectual and Developmental
Disabilities
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
Rebecca R. Kammes, Rhonda S. Black, and Trisha Easley
Abstract
This study used a community-based participatory research approach to examine what
adults with intellectual and developmental disabilities (IDD) view as important topics in
sexuality education. A thematic analysis was conducted on questions written by adults
with IDD regarding sexuality after attending a sexuality education group. Results were
checked for accuracy using a community focus group. Findings provide direct implications
for community-based sexuality education programs for adults with IDD, demonstrating
the need for mentoring regarding authentic relationship experiences as well as
developmentally appropriate sexual health information. Programs need to focus on
helping adults with IDD navigate these interpersonal experiences. This study also
demonstrates the importance of including the voices of adults with IDD in research in
order to ensure its applicability and acceptability.
Keywords: community-engaged, sexuality, intellectual and developmental disabilities
Socialization and sexuality play a unique and and future interpersonal relationships of all people
fundamental role in adult experiences and are (Klein, 2015), proper sexuality education is lacking
important to well-being and quality of life for all even among the general school-age population
people (Diamond & Huebner, 2012; Knox & (Barr et al., 2014). In special education curricula
Hickson, 2001). However, for adults with intellec- specifically, sexuality education is often skipped or
tual and developmental disabilities (IDD), sexual- minimally covered (Brown & McCann, 2018).
ity and romantic relationships are often Barnard-Brak et al. (2014) found that 56% of
overlooked or actively avoided topics (Fulford & students with IDD with mild levels of impairment
Cobigo, 2018). Service providers, parents, and and 84% of students with IDD with moderate to
other caregivers of adults with IDD frequently profound levels of impairment had not received
avoid discussions about relationships and sexuality sexuality education. Sometimes this is due to the
(Evans et al., 2009), and discourage these adults stigmatization and fear of normative sexual
from engaging in sexual relationships (Black & behaviors within this population. Barnard-Brak
Baker, 2013; Black & Kammes, 2019; Fitzgerald & and colleagues (2014) also found that 60% of
Withers, 2011). Additionally, education on these teachers believed that those with IDD with mild
topics is frequently disregarded in favor of levels of impairment could benefit from sexuality
educational programs such as daily living skills education, but only 25% of teachers believed
or employment, despite the essential role relation- those with IDD with moderate to profound levels
ships play in adult independent living (Chrastina of impairment would benefit. Ballan (2012) found
& Vecerova, 2020). that specifically regarding adults with IDD,
Despite the benefits that social and sexual parents and professionals perceived sexuality
health education has on both individual health education as potentially dangerous due to the
2 Sexuality Questions of Adults With IDD
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
myth that individuals with IDD are either asexual, ships (Yankah, 2015). This research has extended
or oversexed and lacking control. They expressed ramifications for individuals with IDD as they
concern that many young people with IDD may transition into adulthood, as it can lead to
(a) have difficulty with discernment, (b) not fully isolation, loneliness, and an increase in negative
comprehend sexuality education information, (c) mental health symptoms (Fulford & Cobigo,
overgeneralize the information, and (d) struggle 2018; Prohn et al., 2019). It also may be a
with understanding the reality of sexuality experi- contributing factor to recent findings based on
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
ences. Parents also expressed concerns that misun- U.S. Department of Justice data that people with
derstandings could lead to increased vulnerability. IDD are sexually assaulted at a rate of more than
Although they felt comfortable talking about seven times of that of people without disabilities
hygiene, grooming, and abuse prevention, they (Shapiro, 2018). The young person with IDD
did not feel comfortable talking to their child with typically has not had dating or intimate relation-
IDD about dating, relationship development, ship experiences, or their experiences have been
intercourse, or birth control. Similarly, Stein and abusive or dependent. Additionally, perpetrators
colleagues (2018) found that most parents ap- of this abuse have typically been peers (other
proved of some form of sexuality education for individuals with IDD) or caregivers (Gill, 2015).
their children but felt more comfortable with Most abuse goes unreported, as individuals with
biology-based education. IDD often do not have the words to express what
Parents play a critical and influential role in has happened or they are not believed when they
the sexuality education and socialization of all do report. Sexuality education can give them
children (Shtarkshall et al., 2007). Parent beliefs words to articulate their experience and concerns
regarding sexuality education for their child with (Ward et al., 2010).
IDD translate into sexuality knowledge and Identifying a healthy, as opposed to abusive,
experiences. Research has found in tests of sexual relationship is difficult for any young adult but is
knowledge that participants with IDD scored well even more difficult for a person with IDD (Coyle,
on questions about anatomy and puberty, but 2016). A lack of sexuality and relationship
had limited knowledge on safe sex practices, education coupled with impoverished social
contraception, sexually transmitted infections, networks contributes to this lack of discernment
and legal issues regarding rights and behaviors (Brown & McCann, 2018). These adults lack peers
(Galea et al., 2004; Jahoda & Pownell, 2014). with whom they can discuss common relationship
Frawley and Wilson (2016) also found that young concerns such as boundaries and respect, which is
people with IDD were more aware of facts how typically developing young adults frequently
regarding sexuality and health, but distinctly gain information (Sun et al., 2018). Young adults
lacked applicable knowledge on relationships with IDD rely on parents and educators for
and sexual interactions. Gil-Llario and colleagues sexuality and intimate relationship information,
(2018) questioned 360 adults with IDD and however these individuals often avoid the topic
found that 89.4% of participants were unhappy assuming someone else will take on the responsi-
with their previous sexuality education and bility (Chrastina & Vecerova, 2020). A compound-
desired further conversation around sexuality ing factor is that many people with IDD are lonely
and general sexual health knowledge. or isolated (Callus, 2017). Isolation, loneliness,
Despite an increase in sexual health education and overprotection can lead to vulnerability for
resources and curricula, many students with IDD abuse (Coyle, 2016), and one of the best ways to
still leave high school without receiving any type stop sexual assault is to teach individuals how to
of sexuality education due to lack of access to identify abuse and recognize healthy relationships
these resources (Treacy et al., 2018) as well as being (Shapiro, 2018). Despite increased vocational
excluded from this component of general educa- programs aimed at expanding previously unmas-
tion (Curtiss, 2018). This finding is alarming tered skills, there is still a distinct lack of
considering that in typically developing popula- appropriate and applicable sexual health educa-
tions sexuality education has been found to have tion for adults with IDD (Richards et al., 2006).
significant positive impacts on sexual health The purpose of this study was to directly
behaviors (Kirby et al., 2005), as well as to engage community partners who were invested in
cultivate positive attitudes towards multiple as- this topic to examine the actual sexuality educa-
pects of personal health and romantic relation- tion needs of adults with IDD. This study
R. R. Kammes, R. S. Black, and T. Easley 3
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
included gaining insight into sexuality education with them to allow for a deeper exploration of
experiences and questions adults with IDD lived experiences (Schmidt, 1993). This study
themselves had regarding sexual health and progressed in three distinct phases that included
relationships they wished were addressed in integrated community collaborations on research
educational groups. Those who work with them that guided their teaching and learning while also
in their community were also included. Our goal generating scholarship for wider audiences
was to interact directly with community members, (Jameson et al., 2011). The first phase included
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
gain their perspectives, and include them in all connecting and collaborating with the commu-
aspects of the research process. A participatory and nity partners to discuss presenting concerns and
emancipatory framework guided the study (Chap- create the research questions. Following Institu-
pell, 2000). Such a framework has at its core that tional Review Board approval, in the second
research should (a) be a tool for improving the phase data were gathered and a team of
lives of people with disabilities; (b) provide more researchers analyzed the data to determine
opportunities for those with disabilities to partic- themes and initial results. In the final phase, a
ipate in all phases of the research; and (c) serve to panel of community members reviewed the
form alliances among people with disabilities, initial results and provided feedback to further
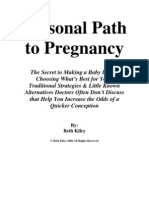
researchers, and other experts (Chappell, 2000). describe and finalize the results. Figure 1 provides
an overview of the three phases of the study.
Method
A community-based participatory research (CBPR) Phase 1: Community Collaboration and
approach was selected for this study (Doberneck et Research Questions
al., 2010; Israel et al., 1998). CBPR methodologies During the first CBPR phase, the research team
provides a direct reciprocal partnership between connected with a local nonprofit organization to
academic researchers and community stakeholders discuss their concerns and issues regarding sexual-
that effectively builds a stronger capacity for
change within the community while providing
implications from research that are directly
applicable to wider audiences (Israel et al., 2010;
Powell & Takayoshi, 2003). CPBR allows for
further empowerment of people and groups by
enhancing their voices and power in society, and
facilitating further social change (Tremblay et al.,
2017). Through this design, community partners
are involved in all aspects of research including
determining research questions, as well as collect-
ing and analyzing data (Israel et al., 1998). Data
collection and analyses are completed in methods
most aligned with the community partners’ values
and functioning of the community. These meth-
ods give the community ownership over the
research and allow results to be community-
situated, collaborative, and action-oriented (Do-
berneck et al., 2010; Israel et al., 2006; Ochocka et
al., 2010). This is especially important when
discussing intervention-related research (Waller-
stein & Duran, 2010).
CBPR engages community and academic
partners in a common knowledge production
process aimed at improving the well-being of
community partners (Tremblay et al., 2017). In
this study, CBPR was used to amplify the voices Figure 1. CBPR Study Phases: Data Collection,
of adults with IDD and those who work closely Analyses, and Interpretation Procedures.
4 Sexuality Questions of Adults With IDD
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
ity education for adults with IDD. Through further questions they had. Participants were able
meetings, members of this organization were able to write these questions themselves, or they could
to specify their concerns and begin to identify verbally relay them to facilitators who would write
potential areas in which action needed to be taken a question card for them. Facilitators would
(Powell & Takayoshi, 2003). During this phase, the attempt to answer these questions during the next
research team learned more about the organiza- session, but indicated they often ran out of time
tion, specifically their sexuality education pro- and were unable to do so. If unable to cover it in
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
gram, and they discussed areas in which they session, they would follow up with participants
could collaborate. individually. Question cards from these seven
different SHARE groups were collected and saved
Community Partners by facilitators. Through collaborative discussion,
A main component of CBPR is the inclusion of these question cards were determined to be a
community partners in all aspects of the research. potential avenue for resources and data (Gust &
The community partners were all associated with a Jordan, 2006).
nonprofit organization in a midwestern state that
provides services for adults with IDD in the areas Research Questions
of sexuality education, social skill acquisition, and Three research questions were developed in direct
employment soft skills training. They work with collaboration with and driven by the community
approximately 250 adults (over the age of 18) each partners (Sandmann, 2006) and were designed
year. This partner organization structures their specifically for adults with IDD who have taken a
services around the belief that education and sexuality education course developed for adults:
enrichment are lifelong needs and their goals are
to promote personal independence and encourage 1. In what sexuality education topics do adults
work within the community. still have gaps in knowledge?
2. What types of questions do adults continue
The Sexual Health and Relationship to have unanswered?
Education Program 3. What are the areas of sexuality education for
The Sexual Health and Relationship Education adults with IDD specifically that need to be
(SHARE) curriculum that was developed by one covered more thoroughly or in different
of the founders of the nonprofit organization was ways?
used to provide sexuality education to the adults
with IDD whom they serve. Participants met in
small groups once a week for 12 weeks. The Phase 2: Analysis of the Question Cards
average group size was seven adults with IDD and During the second CBPR phase, the research
two facilitators. In order to be flexible to the team analyzed the question cards that the
various needs of different groups of participants, facilitators had collected. All questions cards
the curriculum covered one topic each week and used in the analyses had been collected prior to
included a collection of resources for facilitators to beginning Phase 1 of the study, therefore not
use depending on the developmental level and influencing what participants wrote on their
previous sexuality education level of the partici- cards. The research team included a member
pants in the group. See Table 1 for session topics who was an expert in the field of sexuality
and examples of content covered. All the topics in education for adults with IDD and educational
the curriculum were covered throughout the and therapeutic group instruction with 8 years of
program, but the depth that each topic is taught experience. The second research team member
for each group is based on the facilitators’ was an expert in the field of sexuality and special
determination of the appropriateness of the education with 20 years of experience in con-
material. The SHARE program has been run with ducting research and delivering interventions
nine different cohorts. related to sexuality. The third member of the
For the most recent seven cohorts, the same research team was a doctoral student in the area
two SHARE facilitators implemented a teaching of rehabilitation counseling. No member of the
tool they called question cards. After each session, research team was involved in the creation or
participants were provided index cards to ask any implementation of the SHARE program.
R. R. Kammes, R. S. Black, and T. Easley 5
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
Table 1
SHARE Session Topic and Example of Content Covered
Session Topic Example of Content Covered
1. Introduction to the Group Ice breakers and personal introductions
2. Anatomy & Reproductive Systems Male vs. female reproductive systems
3. Puberty, Sexual Health & Hygiene Secondary sex characteristics, menstruation
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
4. Puberty, Sexual Health & Hygiene Part II Bathing, shaving
5. Sex Vaginal and anal intercourse
6. Contraception, Birth Control & Pregnancy Condoms, birthing process
7. Sexual Abuse, Exploitation, & Law Enforcement Consent and abuse/exploitation definitions
8. Sexual Abuse, Exploitation, & Law Enforcement Part II Local laws regarding perpetrator behaviors
9. Types of Relationships Dating vs. long-term relationships
10. Stress & Anxiety in Relationships Recognizing anxiety & depression symptoms
11. Making Friends & Dating Acquaintance vs. friendship vs. dating
relationships
12. End of Group Party Knowledge game and celebration
SHARE Participants participants as a group with no identifiable
Thirty-three adults with IDD (28 males, 5 information provided. The team analyzed the
females) participated across the seven SHARE question cards using a constructionist thematic
groups. Participants were aged 20–52 (M ¼ 29.12, analysis approach (Braun & Clarke, 2006). Analyses
SD ¼ 8.87). Most participants (21; 64%) had a were conducted across two levels of coding: a
diagnosis of autism spectrum disorder (ASD) and semantic categorical analysis and a latent analysis to
IDD with mild levels of impairment. Five examine underlying ideas and conceptualizations.
participants (15%) had a diagnosis of emotional During the first coding level, the research
impairment and IDD with mild levels of team coded all question cards semantically using a
impairment, and seven participants (21%) had a categorical coding system based on Blanchett and
diagnosis of IDD with mild levels of impairment Wolfe’s (2002) review of sexuality education
or cognitive impairment. Most participants lived curricula for individuals with IDD. Their list of
at home with a caregiver (70%), some lived in curriculum concepts was used to categorically
community supported living arrangements code the question cards. Table 2 provides a
(15%), and some lived independently in the comprehensive list of these codes. All members
community (15%). Many of the participants were of the research team independently coded all
employed (36%) or going to school (27%). question cards. All applicable codes were applied
Twelve of the participants (36%) were currently to each question card, as some cards fell into
not employed or attending any school or multiple categories. After the initial independent
vocational program. We do not have information round of coding, the research team met and
on race/ethnicity and current relationship status discussed coding disagreements until consensus
because the organization did not collect that was reached. These codes were then tallied to
information from participants of their services. provide information regarding what sexuality
education curriculum topics were asked about.
Data Analysis During the second level of coding, the
The research team received all collected question research team analyzed all question cards at the
cards (87 total) for analysis. Participants did not latent level for underlying ideas and concepts. All
write any identifying information on the cards, three researchers had previously become familiar
therefore their identities were kept confidential. with the data through the first level of categorical
The cards were also collected and grouped by coding. They then read through all of the question
cohort, but to which cohort each group of cards cards independently and generated codes and
belonged was not identified. The research team also themes they felt were omitted through the first
received demographic information for SHARE level of coding. The research team then met to
6 Sexuality Questions of Adults With IDD
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
Table 2 results were merged with the results of the
Sexuality Education Curriculum Topics Coding categorical analysis to provide a more thorough
Categories understanding of the data.
1. Biological & Reproductive
Anatomy and physiology
Phase 3: Gathering Community Partner
Gender differences Feedback
During the final CBPR phase, the research team
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
Pregnancy
met with a panel of individuals from the
Birth control
community partners to discuss the results of the
2. Healthy & Hygiene question card analyses. The community panel was
Hygiene given the results and asked to provide feedback to
Health and wellness (a) add a deeper explanation of the results,(b)
Alcohol and drug use ensure the results were realistic and applicable to
STD/HIV prevention the community, and (c) negate any potential
STD epidemiology inherent biases the research team may have
Body and disease (Chambers, 2006; Schmidt, 1993). The commu-
nity panel was only given access to the results of
3. Relationships the analyses to provide experience- and opinion-
Relationships/social skills based feedback and did not conduct any analyses
Responsibility to partner themselves. The feedback from the panel was then
Family types and roles integrated to the original results to provide the
Feelings and expressions finalized results of the study.
Dating and marriage
Parenting Community Panel Participants
Sexual orientation The community panel consisted of seven individ-
4. Self-Protection/Self-Advocacy uals. The first panelist was the executive director of
the organization which runs the SHARE program.
Protection against abuse
The second panelist was the creator of the SHARE
Sexual feelings
program and the original facilitator. The third
Sexuality as positive aspect of self panelist was a female SHARE facilitator with a
Sexual behavior other than intercourse background working as a direct service personnel
Appropriate and inappropriate touching for adults with IDD. The fourth panelist was the
Decision making second female SHARE facilitator who was cur-
Use of condoms rently a master’s student in rehabilitation counsel-
Reduction of fear and myths ing. The fifth panelist was an adult female with
Personal rights ASD who had previously participated in the
Sexual discrimination SHARE program. The sixth panelist was an adult
Saying ‘‘no’’ to sex female with IDD with mild levels of impairment
Saying ‘‘no’’ to drugs who had previously participated in the SHARE
Saying ‘‘no’’ to alcohol program. The final panelist was an adult male with
Saying ‘‘no’’ to tobacco ASD who had not taken the SHARE program but
Note. Coding categories taken from Blanchett & Wolfe
had received a sexuality education course in high
(2002). school. Using a CBPR framework (Doberneck et
al., 2010) it was important to include those
discuss and agree upon the thematic codes. The directly connected to the SHARE program in
the focus groups as their experiences would
team then returned to the data independently and
provide the research team with the most applica-
coded all question cards based on the finalized ble feedback to ensure accurate results. It was also
codes. Finally, the team met again and discussed important to include adults with IDD in the panel
any coding disagreements until consensus was to ensure the inclusion of all community partners
reached. These codes were then tallied and the (Bigby et al., 2014). Demographic information
R. R. Kammes, R. S. Black, and T. Easley 7
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
(e.g., age, race, education level) were not collected Results
for the panel.
The results of the study provided two overarching
themes: authentic relationship experiences, and
Community Panel Feedback individual sexual health knowledge. The first
The panel received only the summarized results of theme includes the desire to further their
the question card analysis; no examples of cards knowledge about authentic relationship experi-
were given to ensure the de-identification of the
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
ences. This theme also contains three subthemes:
data throughout the study. The panel was asked to social norms, sexual behaviors outside of inter-
gather their initial thoughts along with answers to course, and communication within relationship.
three specific reflection prompts: The second theme includes the need for con-
1. Could the timing of when the question cards tinuing discussion of general individual sexual
were collected have impacted the results of health knowledge.
the study?
2. Please provide specific feedback on the new Theme 1: Authentic Relationship
themes of social norms, sexual behaviors Experiences
outside of intercourse, and communication The first theme is that of participants desiring
within relationships. further knowledge and information on authentic,
3. What are potential concerns with the format real-world relationship experiences. During the
of how SHARE presents these topics? first round of coding, the majority (93%) of
participant questions were coded as belonging in
Two focus groups were then conducted to
either the relationship focused or self-protection/self-
gather feedback (Krueger & Casey, 2015). During
advocacy categories of the sexuality education
each focus group, the participants were asked the curriculum topics review (Blanchett & Wolfe,
three reflection prompts, and then were asked to 2002). This result indicated a desire from partic-
provide any additional open-ended feedback ipants to understand how the information they
regarding the results. The first focus group received in the sexuality education course trans-
consisted of the executive director of the lated to real-world experiences. Examples of
organization, the creator of the SHARE pro- relationship-focused questions included, ‘‘Does
gram, and the two SHARE facilitators. This sex need to be central to a relationship?’’ and
focus group lasted 1.5 hr. The second focus ‘‘How to know when you are ready to get into bed
group consisted of the executive director and the with your girlfriend for the first time?’’ Examples
three adults with IDD. The executive director of questions regarding the self-protection/self-
did not participate in the feedback portion of advocacy category included, ‘‘How do you handle
this group and was only there to make the other peer pressure?’’ and ‘‘Why are females more often
participants feel comfortable and to help them victims of sexual assault than males?’’ The results
clarify their feedback as needed. This focus from the community panel indicated that al-
group lasted 2 hr. though these topics were covered as part of the
The strong relationships established between curriculum, facilitators recognized that they did
the research team and all the community partners not cover the topics in depth like they did other
during Phase 1 of the study enabled those who topics (e.g., sexual hygiene, safe-sex practices,
participated in the focus group to feel more sexual anatomy). They specified that the topic of
comfortable. Feedback from all groups was audio relationships is difficult to cover because it
recorded. Two members of the research team requires discussions of personal values, gray areas,
listened to the audio recording, summarized the and individual desires that are difficult for
feedback, and then met to discuss and finalize it. facilitators to discuss in a group setting. One
This information was then merged with the results panelist stated, ‘‘It’s the issue of participants
of initial question card analysis for finalized needing more ‘black and white’ answers, but these
results. The panelists conducted a member check aren’t really that way, so that’s why the adults have
of the finalized results (Lincoln & Guba, 1985). so many questions about them.’’ Because of these
The panelists did not add or change anything, and concerns, more emphasis is placed on other
all agreed with the results. sexuality topics within the curriculum.
8 Sexuality Questions of Adults With IDD
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
Social Norms worry about potential issues if caregivers with
The subtheme of social norms refers to questions guardianship of participants have concerns with
regarding general societal expectations about what they are teaching. Facilitators recognize that
relationships. In these questions, participants this is a topic area that could be a divisive issue for
expressed concern about what they should expect many caregivers, and they avoid the topic in order
as they date or enter into a long-term relationship, to avoid those concerns.
as well as whether they would be able to meet the
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
expectations of others. Examples of this type of Communication Within Relationship
question included, ‘‘What are the rules of This subtheme refers to specific questions regard-
texting?’’ and ‘‘Is it right to date someone at least ing communication expectations within relation-
10 years older/younger than you?’’ Some of these ships and includes how to talk with dating partners
questions were disability-specific, for example one about sexual preferences, previous experiences,
participant with ASD questioned, ‘‘Is it possible and sexual expectations. Related to this category,
that I might get a rejection from other people, participants asked, ‘‘When do you know when it is
because of the fact that I have autism?’’ the right time in a relationship to start having
Questions in this category also showed a sex?,’’ ‘‘I remember hearing a phrase ‘I would
concern for integrating information they have never date someone who has had more sexual
heard from siblings, peers, and the media, and partners than me.’ How do I know?,’’ and ‘‘How
being able to discern between phrases that are do you handle dating around when you have trust
social clichés compared to real expectations. As issues?’’ Some of these questions were also
these participants enter adulthood, they find regarding how to determine explicit compared to
themselves either in romantic situations or have implicit communication and rules within the
friends and siblings who are in romantic situa- relationship. One participant listed ‘‘consent v.
tions, and so their awareness and questions non-consent with drinking and how to know’’ as a
become more focused on understanding the topic they wanted to know more about.
social norms they encounter during these expe-
riences. For example, one participant asked, ‘‘The Theme 2: Individual Sexual Health
joke is a man will last a minute. So actual sex is
not like a porn video. Will my partner under-
Knowledge
The second theme is participant questions related
stand that?’’ Another participant echoed this
to their own sexual health that are not specifically
sentiment asking, ‘‘What is actually the average
asked within a relationship context. During the
length of intercourse?’’
first round of coding, only 49% of participant
questions were coded as belonging in either the
Sexual Behaviors Outside of Intercourse biology and reproductive or health and hygiene
This subtheme related to specific questions categories of the sexuality education curriculum
regarding a wider range of sexual behaviors outside topics review (Blanchett & Wolfe, 2002). This
of the biological act of intercourse including issues finding indicated that although participants still
such as oral sex, self-stimulation, and foreplay had questions regarding these topics, they were
behaviors. Examples of questions from partici- fewer in comparison to questions regarding
pants included, ‘‘Is it ok to masturbate while in a authentic relationship experiences.
relationship?,’’ ‘‘Can you have oral sex with Overall, the category of health and hygiene had
condoms?,’’ and ‘‘Can you hold off on an the fewest questions (12%). Examples of health
orgasm? How?’’ These questions were sometimes and hygiene questions included, ‘‘What is toxic
also related to social norms and what is to be shock?,’’ ‘‘What lubricant is healthy to use for
expected in authentic relationship experiences, sex?,’’ and ‘‘Should women wear a bra when they
such as ‘‘Is sex addiction real?’’ Sexual intercourse sleep at night?’’ The community panel provided
is covered in the SHARE curriculum, but other insight into this. One panelist stated, ‘‘Hygiene
sexual behaviors are often not discussed. The seems to be more addressed actually in session and
community panel indicated that this as a very it also might be easier for participants to ask about
difficult area to teach, specifically because of the it in person so that is why they don’t have as many
impact that personal values have on potential cards.’’ Another panelist and SHARE facilitator
answers to these questions. They also indicated noted, ‘‘The SHARE program always teaches these
R. R. Kammes, R. S. Black, and T. Easley 9
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
topics first, so there is probably more energy indicated that adults with IDD know what types of
around this because of that. Plus, it’s not as questions to ask and understand the types of
embarrassing since the same information basically information they desire, sexuality education should
applies to everyone.’’ be implemented accordingly.
The biology and reproductive category had more The results of this study also indicated that
questions than health and hygiene, but still fewer adults with IDD still have questions related to
than those related to authentic relationship general sexual health knowledge (e.g. anatomy and
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
experiences (33%). Examples of questions partic- physiology). This finding is consistent with the
ipants asked included, ‘‘Does the mother get findings of Schaafsma and colleagues (2015) that
scratches when giving birth to the baby?,’’ repetition, rehearsal, and practice over time are the
‘‘During ovulation how much does the women’s most effective methods for teaching sexuality
temp go up?,’’ and , ‘‘What exactly does the education to individuals with IDD. This study
prostate do?’’ Feedback from the panel indicated indicates that adults feel they need a review of this
that there may be more questions regarding this information specifically as it relates to their
topic due to the tangible nature of the informa- developing adult bodies. Addressing this gap
tion. One panelist noted, ‘‘These topics overall are may be difficult to do as groups are often
more tangible and concrete, so they’re probably comprised of adults with many different levels of
easier to ask about.’’ The information may be previous experience in sexual health education, so
easier for participants to integrate the knowledge it would be important to assess the knowledge of
and have specific questions. A panelist who was the group before beginning to determine what
also an adult with IDD noted ‘‘This is the only topic areas need to be covered. These topics are
thing they really taught me in school. So, it’s nice often easy to cover in a didactic training model
to hear it again because now I know what and can most likely be easily implemented in any
questions to ask. But I don’t have many because adult sexuality education course.
I’ve learned more over the years.’’
Limitations of the Study
Discussion One limitation of this study is that the SHARE
This study resulted in two themes regarding program did not follow a specific evidence-based
sexuality education for adults with IDD. The first curriculum. Because of this, no treatment fidelity
theme was authentic relationship experience knowl- checks were conducted and therefore we cannot
edge and information, and the second theme was determine the exact content each group of partic-
content related to individual sexual health knowl- ipants received. However, for the purposes of this
edge. Adults with IDD expressed a desire for study, the researchers had access to all curriculum
information regarding authentic relationship expe- materials and it was determined that the program
riences. They wanted to further understand how to covered the same components as most sexuality
integrate this information into their own personal education curricula described in the research
experiences, as well as to know what types of literature (Blanchett & Wolfe, 2002). Although the
experiences they should be expecting. The com- lack of using an evidence-based curriculum may
munity panel helped explain that this information have had an impact on the study results related to
was difficult to cover because of the ambiguous content covered in the SHARE program, it is a
nature of the topic. This topic may be more suited common reality that many nonprofit adult pro-
to a coaching and mentoring style of teaching, as grams are unable to purchase and access most
opposed to the dyadic instruction that is common sexuality education curricula. And although many
in most sexuality education groups. Adults with free curricula do exist, most of them are aimed
IDD demonstrated a desire to engage in relation- towards adolescents and young adults and materials
ship experiences but need further guidance and often need to be supplemented for adults.
explicit instruction in putting this information into In relation to the use of an organization-
practice (Galea et al., 2004). Safety and self- specific curriculum, it should be noted that the
protection related to these experiences should be community panel consisted mainly of people who
integrated into education in a manner related to were directly aligned with the use of this
healthy relationships as opposed to simply avoiding curriculum. Due to this factor, they were not
abuse (Ward et al., 2013). Because this study included in the analysis of the question cards,
10 Sexuality Questions of Adults With IDD
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
which may have influenced their interpretation of marry, as well as multiple other barriers these
the results during the focus groups. adults experience in having relationships (Black &
Another limitation of the study is that most Kammes, 2019). Including components of coach-
adults with IDD who participated in the SHARE ing and mentoring will also help adults with IDD
program were males which is potentially connect- directly apply that knowledge to their own
ed to a high rate of ASD among participants and experiences (Gilson & Carter, 2016; Walker et
that males are more commonly diagnosed with al., 2016). For adults, sexuality education is more
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
ASD than females (Adamou et al., 2018). This than the instruction of anatomy and sex. It needs
limitation could potentially impact the results of to include an understanding of the inner-self
the study in relation to questions asked, as male within the context of the outer-world. This
and female adults may have different areas of initiative would be aided by including further
interest in sexuality, as well as potentially receiving materials regarding sexual identity and sexual
different levels of sexuality education previously orientation (Bedard et al., 2010; L öfgren-
(e.g., females often receive more abuse avoidance Mårtenson, 2009; Noonan & Taylor Gomez,
information socially than males; Radin, 2017; 2011). It is important to note that objective
Scriver & Kennedy, 2016). sexuality education topics (i.e., health and hy-
Regarding the question cards, a limitation of giene, anatomy and physiology) continually and
their use is in the de-identification process that was progressively need to be covered at a developmen-
used. We were unable to tell who wrote the cards or tally appropriate level with multiple examples for
even which cohort the cards came from. Due to individuals with IDD (Schaafsma et al., 2015).
this, we are unable to tell if cards were evenly Adults with IDD benefit most from direct and
distributed across participants or if there were some literal examples and information. The type and
who disproportionally asked more questions. need for information develop as individuals age.
A final limitation is the number of partici- Often adults of varying disability levels are
pants. The small group of adults with IDD who placed into the same groups due to lack of funding
participated in these groups also limits the for multiple groups. These groups are impacted by
generalizability of the study. This study is meant facilitators’ lack of knowledge on the difficulties of
to be an introductory CBPR study to begin having different ability levels in one group, and
elevating the voices of adults with IDD in their overall lack of adult community-based program-
own sexuality education and offering innovative ming for these adults (Ward et al., 2013). This has
ways to collect research data from these adults. negative impacts on the ability of the adult to
improve overall, as well as on their ability to apply
self-determination (Brown & McCann, 2018;
Implications for Practice Glen, 2015). It is important to provide adults
Results of this study provide direct implications with IDD with ‘‘real-world’’ advice and examples,
for community-based sexuality education pro- especially related to social norms, their own sexual
grams for adults with IDD with regard to behaviors, and communication within interper-
understanding what topics are important to them, sonal relationships.
and identifying the most common knowledge Sexuality is personal and the social nature of
gaps. In order to support further inclusion of relationships are difficult topics to discuss. The
people with IDD within society, these programs more conversations in which adults with IDD can
need to be learner-centered and place more of an engage on the topics of sexuality and relationships,
emphasis on helping adults integrate and apply the less anxiety and uncertainty they will likely
knowledge regarding everyday relationship experi- experience. Sexuality education providers should
ences. Sexuality education for adults with IDD deliver reliable emotional support and guidance to
should be conducted within a healthy relationship foster a supportive open environment to discuss
context. Groups specifically designed for adults any topic a participant may inquire about. It is
with IDD should be focused on advocating for the important to feel that discussions will not be
adult’s need for information that is essential to judged by those in a position of power as an
more authentic and impactful personal experienc- educator. It is crucial that the staff is comfortable
es and directly applicable to their lives. This group discussing sexuality and relationships. Staff need
design would include information that considers training in how to explain the complexity of
different living situations, the potential inability to sexuality within the context of relationships. It is
R. R. Kammes, R. S. Black, and T. Easley 11
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
also important to consider the gender of the not being covered in the manner necessary for these
facilitator in comparison to participants for these individuals. There is a direct need for policy change
groups, as participants may be more comfortable regarding sexuality education in K-12 schools,
discussing sexuality with an individual who they especially in regard to the inclusion of individuals
relate to with regard to gender (Harrison & Ollis, with IDD and incorporating this information into
2015; Mannix et al., 2010). special education classrooms as well.
Due to the directly applicable nature of the
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
CBPR study design (Powell & Takayoshi, 2003), Future Research With Adults With IDD
the SHARE program has already used the results This study amplifies the importance of including
to create a sequential model for their program. In the voices of adults with IDD in research in order
this model, adults must first take SHARE 1, which to ensure its applicability and acceptability (Beail
focuses on individual sexual health using didactic & Williams, 2014; Caldwell, 2014). The CBPR
instruction and group education practices. After process specifically could further promote the
the completion of SHARE 1, participants are inclusion of adults with IDD, as the use of CBPR
eligible to take SHARE 2 which focuses on methods provides a more inclusive way to address
healthy sexuality within a relationship context health disparities among underrepresented com-
using didactic instruction, group therapy tech- munities (Sandoval et al., 2012). Having adults
niques, and personal coaching. with IDD engage in the research process beyond
simply as participants provides them with more
Policy Implications ownership in directly addressing issues that are of
The results of this study indicate the need for concern to them (Shogren & Wehmeyer, 2015).
policy change in how sexuality education is This is especially true for the topic of sexuality and
embedded into transition programs. It would be with recent advances in initiatives for adults with
helpful to embed sexuality education first within disabilities to engage in sexual self-advocacy
transition programs prior to exiting compulsory (English et al., 2018; Fulford & Cobigo, 2018;
schooling, and then in community-based voca- Whittle & Butler, 2018). Sexuality in general is a
tional and adult day programs. Sexuality is a large difficult topic to discuss, and researchers need to
component of adult life and experiences and continue to find different ways to help partici-
integrating this information within other program- pants discuss these issues and concerns.
ming would help adults with IDD to examine the This study also points to the need for
systemic nature of these issues and understand continued research into evaluating sexuality educa-
relationships within a broader cultural and expe- tion programs to ensure they are meeting the needs
riential context. of the individuals they are intended to serve. The
The CBPR methodology used in this study also community panel in this study indicated difficulties
underscores the importance of continuing to in finding a sexuality intervention program that was
conduct research on the topic of sexuality with the applicable to the population of aging adults with
population of adults with IDD. There currently IDD. These programs may already exist, and
exists limited available grant funding for CBPR researchers need to continue to evaluate them and
research. The results of this study show the make them available to the public.
importance of conducting CBPR research to ensure
practices are applicable and acceptable to the Conclusion
individuals they are meant to be servicing. Funding
CBPR projects would allow adults with IDD more This study used CBPR methods to discover what
opportunity to engage in supported decision making types of questions adults with IDD have regarding
that could also impact policy and programming. sexuality education and what topic areas continue
This study also has implications for altering to be of concern in adulthood. It was discovered
policy to require schools to incorporate inclusive that participants wanted more information regard-
and meaningful sexuality education for individuals ing authentic relationship experiences, and desired
with IDD in Grades K-12. It is a disservice to more developmentally appropriate information
individuals with IDD to wait until adulthood to regarding ageing. Adults with IDD also need
receive appropriate sexuality education, especially if access to information and mentorship regarding
basic concepts such as anatomy and physiology are relationship experiences that facilitate safe com-
12 Sexuality Questions of Adults With IDD
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
munity integration including helping them under- supports for youth with IDD (pp. 83–119).
stand what to expect and guiding them through National Association of the Dually Diagnosed
current experiences. Future research and practice (NADD) Press.
should continue to examine appropriate methods Black, R. S., & Kammes, R. R. (2019). Restrictions,
for implementing sexuality education and ensure power, companionship, and intimacy: A
the inclusion of the voices of adults with IDD in meta-synthesis of people with intellectual
both research and practice. disabilities speaking about sex and relation-
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
ships. Intellectual and Developmental Disabilities,
57(3), 212–233.
References Blanchett, W. J., & Wolfe, P. S. (2002). A review
Adamou, M., Johnson, M., & Alty, B. (2018). of sexuality education curricula: Meeting the
Autism diagnostic observation schedule sexuality education needs of individuals with
(ADOS) scores in males and females diag- moderate and severe intellectual disabilities.
nosed with autism: A naturalistic study. Research & Practice for Persons with Severe
Advances in Autism, 4, 49–55. https://doi. Disabilities, 27, 43–57. https://doi.org/10.
org/10.1108/AIA-01-2018-0003 2511/rpsd.27.1.43
Ballan, M. S. (2012). Parental perspectives of Braun, V., & Clarke, V. (2006). Using thematic
communication about sexuality in families of analysis in psychology. Qualitative Research in
children with Autism Spectrum Disorders. Psychology, 3, 77–101. https://doi.org/10.
Journal of Autism and Developmental Disorders, 1191/1478088706
42, 676–684. https://doi.org/10.1007/s10803- Brown, M., & McCann, E. (2018). Sexuality issues
011-1293-y and the voices of adults with intellectual
Barnard-Brak, L., Schmidt, M. Chesnut, S., Wei, disabilities: A systematic review of the litera-
T., & Richman, D. (2014). Predictors of access ture. Research in Developmental Disabilities, 74,
to sex education for children with intellectual 124–138. https://doi.org/101016/j.ridd.2018.
disabilities in public schools. Intellectual and 01.009
Developmental Disabilities, 52, 85–97. https:// Caldwell, K. (2014). Dyadic interviewing: A
doi.org/10.1352/1934-9556-52.2.85 technique valuing interdependence in inter-
Barr, E. M., Goldfarb, E. S., Russell, S., Seabert, views with individuals with intellectual dis-
D., Wallen, M., & Wilson, K. L. (2014). abilities. Qualitative Research, 14, 488–507.
Improving sexuality education: The develop- https://doi.org/10.1177/1468794113490718
ment of teacher-preparation standards. Journal Callus, A. M. (2017). Being friends means helping
of School Health, 84, 396–415. https://doi.org/ each other, making coffee for each other:
10.1111/josh.12156 Reciprocity in the friendships of people with
Beail, N., & Williams, K. (2014). Using qualitative intellectual disability. Disability & Society, 32,
methods in research with people who have 1–16. https://doi.org/10.1080/09687599.
intellectual disabilities. Journal of Applied 2016.1267610
Research in Intellectual Disabilities, 27, 85–97. Chambers, R. (2006, July). Poverty unperceived:
https://doi.org/10.1111/jar.12088 Traps, biases, and agenda. Working Paper, No.
Bedard, C., Lan Zhang, H., & Zucker, K. J. (2010). 270. Institute for Development Studies.
Gender identity and sexual orientation in Chappell A. L. (2000). Emergence of participatory
people with developmental disabilities. Sexu- methodology in learning difficulty research:
ality & Disability, 28, 165–175. https://doi. Understanding the context. British Journal of
org/10.1007/s11195-010-9155-7 Learning Disabilities, 28, 38–43. https://doi.
Bigby, C., Frawley, P., & Ramcharan, P. (2014). org/10.1046/j.1468-3156.2000.00004.x
Conceptualizing inclusive research with peo- Chrastina, J., & Vecerova, H. (2020). Supporting
ple with intellectual disability. Journal of sexuality in adults with intellectual disability—
Applied Research in Intellectual Disabilities, 27, A short review. Sexuality and Disability, 38,
3–12. https://doi.org/10.1111/jar.12083 285–298. https://doi.org/10.1007/s11195-
Black, R. S., & Baker, D. (2013). Sexuality and 018-9546-8
youth with the dual diagnoses of intellectual Coyle, S. (2016). Children and families forum:
disability and mental illness. In D. J. B. & E. Sex ed for young adults with I/DD. Social
R. Blumberg (Ed.), Mental health and wellness Work Today, 16(2), 34. https://www.
R. R. Kammes, R. S. Black, and T. Easley 13
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
socialworktoday.com/archive/032216p34. Gil-Llario, M. D., Morell-Mengual, V., Ballester-
shtml Arnal, R., & Diaz-Rodriguez, I. (2018). The
Curtiss, S. L. (2018). The birds and the bees: experience of sexuality in adults with intellec-
Teaching comprehensive human sexuality tual disability. Journal of Intellectual Disability
education. TEACHING Exceptional Children, Research, 62, 72–80. https://doi.org/10.1111/
51(2), 134–143. https://doi.org/10.1177/ jir.12455
0040059918794029 Gill, M. (2015). Already doing it: Intellectual
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
Diamond, L. M., & Huebner, D. M. (2012). Is disability and sexual agency. University of
good sex good for you? Rethinking sexuality Minnesota Press.
and health. Social and Personality Psychology Gilson, C. B., & Carter, E. W. (2016). Promoting
Compass, 6, 54–69. https://doi.org/10.1111/j. social interactions and job independence for
1751-9004.2011.00408.x college students with autism or intellectual
Doberneck, D. M., Glass, C. R., & Schweitzer, J. disability: A pilot study. Journal of Autism and
H. (2010). From rhetoric to reality: A Developmental Disorders, 46, 3583–3596.
typology of publicly engaged scholarship. https://doi.org/10.1007/s10803-016-2894-2
Journal of Higher Education Outreach and Glen, K. B. (2015). Supported decision-making
Engagement, 14, 5–35. and the human right of legal capacity.
English, B., Tickle, A., & dasNair, R. (2018). Views Inclusion, 3, 2–16. https://doi.org/10.1352/
and experiences of people with intellectual 2326-6988-3.1.2
disabilities regarding intimate relationships: A Gust, S., & Jordan, C. (2006). The community
qualitative metasynthesis. Sexuality and Dis- impact statement: A prenuptial agreement for
ability, 36, 149–173. https://doi.org/10.1007/ community-campus partnerships. Journal of
s11195-017-9502-z Higher Education Outreach and Engagement 12,
Evans, D. S., McGuire, B. E., Healy, E., & Carley, 155–169.
S. N. (2009). Sexuality and personal relation- Harrison, L., & Ollis, D. (2015). Stepping out of
ships for people with an intellectual disability. our comfort zones: Pre-service teachers’ re-
Part II: Staff and family carer perspectives. sponses to a critical analysis of gender/power
Journal of Intellectual Disability Research, 53, relations in sexuality education. Sex Education,
913–921. https://doi.org/10.1111/j.1365- 15, 318–331. https://doi.org/10.1080/
2788.2009.01202.x 14681811.2015.1023284
Fitzgerald C., & Withers, P. (2011). ‘‘I don’t know Israel, B., Schulz, A., Parker, E., & Becker, A.
what a proper woman means’’: What women (1998). Review of community-based research:
with intellectual disability think about sex, Assessing partnership approaches to improve
sexuality and themselves. British Journal of public health. Annual Review of Public Health,
Learning Disability, 41, 5–12. https://doi.org/ 19, 173–202. https://doi.org/10.1146/
10.1111/j.1468-3156.2011.00715.x annurev.publhealth.19.1.173
Frawley, P. & Wilson, N. J. (2016). Young people Israel, B. A., Coombe, C. M., Cheezum, R. R.,
with intellectual disability talking about Schulz, A. J., McGranaghan, R. J., Lichten-
sexuality education and information. Sexuality stein, R., Reyes, A. G., Clement, J., & Burris,
and Disability, 34, 469–484. https://doi.org/ A. (2010). Community-based participatory
10.1007/s11195-016-9460-x research: A capacity building approach for
Fulford, C., & Cobigo, V. (2018). Friendships and policy aimed at eliminating health disparities.
intimate relationships among people with American Journal of Public Health, 100, 2094–
intellectual disabilities: A thematic synthesis. 2102. https://doi.org/10.2105/AJPH.2009.
Journal of Applied Research in Intellectual Dis- 170506
abilities, 31, 18–35. https://doi.org/10.1111/ Israel, B. A., Krieger, J., Vlahov, D., Ciske, S.,
jar.12312 Foley, M., Fortin, P., Guzman, J. R., Lichten-
Galea, J., Butler, J., Iacono, T., & Leighton, D. stein, R., McGranaghan, R., Palermo, A., &
(2004). The assessment of sexual knowledge in Tang, G. (2006). Challenges and facilitating
people with intellectual disability. Journal of factors in sustaining community partnerships:
Intellectual & Developmental Disability, 29, 350– Lessons learned from the Detroit, New York
365. https://doi.org/10.1080/136682504 City and Seattle urban research centers.
00014517 Journal of Urban Health: Bulletin of the New
14 Sexuality Questions of Adults With IDD
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
York Academy of Medicine, 83, 1022–1040. Ochoka, J., Moorlag, E., & Janzen, R. (2010). A
https://doi.org/10.1007/s11524-006-9110-1 framework for entry: PAR values and engage-
Jahoda, A., & Pownall, J. (2014). Sexual under- ment strategies in community research. Gate-
standing, sources of information and social ways: International Journal of Community
networks: The reports of young people with Research and Engagement 3, 1–19. https://doi.
intellectual disabilities and their non-disabled org/10.5130/ijcre.v3i0.1328
peers. Journal of Intellectual Disability Research, Powell, K. M., & Takayoshi, P. (2003). Accepting
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
58, 430–441. https://doi.org/10.1111/jir. roles created for us: The ethics of reciprocity.
12040 College Composition and Communication, 54,
Jameson, J. K., Clayton, P. H., & Jaeger, A. J. 394–422. https://doi.org/10.2307/3594171
(2011). Community engaged scholarship as Prohn, S. M., Kelley, K. R., & Westling, D. L.
mutually transformative partnerships. In L. (2019). Supports perspectives on the social
Harter, J. Hamel-Lambert, & J. Millesen experiences of college students with intellec-
(Eds.), Participatory partnerships for social action tual disability. Inclusion, 7, 111–124. https://
and research (pp. 259–278). Kendall Hunt. doi.org/10.1352/2326-6988-7.2.111
Kirby, D., Laris, B., & Rolleri, L. (2005). Impact of Radin, M. E. (2017). Sisterhood and sexual assault:
sex and HIV education programs on sexual Engaging sorority members in dialogue, crit-
behaviors of youth in developing and developed ical analysis, and feminist praxis. Family
countries. Family Health International, Youth- Relations, 66, 126–138. https://doi.org/10.
Net Program. 1111/fare.12234
Klein, D. (2015). Knowledge, attitude and behav- Richards, D., Miodrag, N., & Watson, S. L. (2006).
ioral changes as a result of sex education. Sexuality and developmental disability: Ob-
Journal of Sex Education and Therapy, 10, 26– stacles to healthy sexuality throughout the
lifespan. Developmental Disabilities Bulletin, 1,
30.
137–155.
Knox, M., & Hickson, F. (2001). The meanings of
Sandmann, L. R. (2006). Scholarship as architec-
close friendship: The views of four people
ture: Framing and enhancing community
with intellectual disabilities. Journal of Applied
engagement. Journal of Physical Therapy Educa-
Research in Intellectual Disabilities, 14, 276–291.
tion, 20, 80–84. https://doi.org/10.1097/
https://doi.org/10.1046/j.1468-3148.2001.
00001416-200610000-00013
00066.x
Sandoval, J. A., Lucero, J., Oetzel, J., Avila, M.,
Krueger, R.A., & Casey, M.A. (2015). Focus groups: Belone, L., Mau, M., Pearson, C., Tafoya, G.,
A practical guide for applied research (5th ed.). Duran, B., Iglesias Rios, L., & Wallerstein, N.
Sage Publications. (2012). Process and outcome constructs for
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic evaluating community-based participatory re-
inquiry. Sage Publications. search projects: A matrix of existing measures.
Löfgren-Mårtenson L. (2009). The invisibility of Health Education Research, 27, 680–690.
young homosexual women and men with https://doi.org/10.1093/her/cyr087
intellectual disabilities. Sexuality & Disability, Schaafsma, D., Kok, G., Stoffelen, J. M. T., &
27, 21–26. https://doi.org/10.1007/s11195- Curfs, L. M. G. (2015). Identifying effective
008-9101 methods for teaching sex education to indi-
Mannix McNamara, P., Geary, T., & Jourdan, D. viduals with intellectual disabilities: A system-
(2010). Gender implications of the teaching of atic review. Journal of Sex Research, 52, 412–
relationships and sexuality education for 432. https://doi.org/10.1080/00224499.2014.
health-promoting schools. Health Promotion 919373
International, 26, 230–237. https://doi.org/10. Schmidt, M. R. (1993). Grout: Alternative kinds of
1093/heapro/daq046 knowledge and why they are ignored. Public
Noonan, A., & Taylor Gomez, M. (2011). Who’s Administration Review 53, 525–530. https://
missing? Awareness of lesbian, gay, bisexual doi.org/10.2307/977362
and transgender people with intellectual Scriver, S., & Kennedy, K. M. (2016). Delivering
disability. Sexuality & Disability, 29, 175– education about sexual violence: Reflections
180. https://doi.org/10.1007/s11195-010- on the experience of teaching a sensitive topic
9175-3 in the social and health sciences. Irish
R. R. Kammes, R. S. Black, and T. Easley 15
INCLUSION ÓAAIDD
2021, Vol. 9, No. 1, 2–16 DOI: 10.1352/2326-6988-9.1.2
Educational Studies, 35, 195–211. https://doi. science and practice to improve health equity.
org/10.1080/03323315.2016.1146158 American Journal of Public Health, 100, 40–46.
Shapiro, J. (Host). (2018, January 9). For some https://doi.org/10.2105/AJPH.2009.184036
with intellectual disabilities, ending abuse Ward, K. M., Atkinson, J. P., Smith, C. A., &
starts with sex ed. [Audio podcast episode]. Windsor, R. (2013). A friendships and dating
In Special Series: Abused and Betrayed. National program for adults with intellectual and
Public Radio. https://www.npr.org/2018/01/ developmental disabilities: A formative eval-
Downloaded from http://meridian.allenpress.com/inclusion/article-pdf/9/1/2/2779759/i2326-6988-9-1-2.pdf by AAIDD Group A Referring url, Rhonda Black on 02 March 2021
09/572929725/for-some-with-intellectual- uation. Intellectual & Developmental Disabilities,
disabilities-ending-abuse-starts-with-sex-ed 51, 22–32. https://doi.org/10.1352/1934-
Shogren, K. A., & Wehmeyer, M. L. (2015). A 9556-5 1.01.022.
framework for research and intervention Ward, K. M., Bosek, R. L., & Trimble, E. L.
design in supported decision-making. Inclu- (2010). Romantic relationships and interper-
sion, 3, 17–23. https://doi.org/10.1352/2326- sonal violence among adults with develop-
6988-3.1.17 mental disabilities. Intellectual and
Shtarkshall, R. A., Santelli, J. S., & Hirsch, J. S.
Developmental Disabilities, 48, 89–98. https://
(2007). Sex education and sexual socializa-
doi.org/10.1352/1934-9556-48.2.89
tion: Roles for educators and parents. Perspec-
Whittle, C. & Butler, C. (2018). Sexuality in the
tives on Sexual and Reproductive Health, 39,
lives of people with intellectual disabilities: A
116–119. https://doi.org/10.1363/3911607
Stein, S., Kohut T., & Dillenburger, K. (2018). The meta-ethnographic synthesis of qualitative
importance of sexuality education for children studies. Research in Developmental Disabilities,
with and without intellectual disabilities: 75, 68–81. https://doi.org/10.1016/j.ridd.
What parents think. Sexuality and Disability, 2018.02.008
36, 141–148. https://doi.org/10.1007/s11195- Yankah, E. (2015). Evidence-based approaches to
017-9513-9 sexuality education: A global perspective. Rout-
Sun, W. H., Miu, H. Y. H., Wong, C. K. H., ledge.
Tucker, J. D., & Wong, W. C. W. (2018).
Assessing participation and effectiveness of a
peer-led approach in youth sexual health Received 12/15/2019, accepted 7/22/2020.
education: Systematic review and meta-analy-
sis in more developed countries. The Journal of Components of this manuscript have previously been
Sex Research, 55, 31–44. https://doi.org/10. presented orally at the TASH annual conference, the
1080/00224499.2016.1247779 American Association on Intellectual and Developmen-
Treacy, A. C., Taylor, S. S., & Abernathy, T. V.
tal Disabilities annual meeting, as well as the
(2018) Sexual health education for individuals
Engagement Scholarship Consortium annual confer-
with disabilities: A call to action. American
Journal of Sexuality Education, 13(1), 65–93. ence. We would like to extend a thank you of support to
https://doi.org/10.1080/15546128.2017. our commuity-partners, ASPPIRE of Mid-Michigan,
1399492 who were integral part of completing this project.
Tremblay, M. C., Martin, D. H., Macaulay, A. C.,
& Pluye, P. (2017). Can we build on social
movement theories to develop and improve Authors:
community-based participatory research? A Rebecca R. Kammes, Michigan State University;
framework synthesis review. American Journal Rhonda S. Black, University of Hawaii-Manoa, and
of Community Psychology, 59, 333–362. https:// Trisha Easley, Michigan State University.
doi.org/10.1002/ajcp.12142.
Walker, Z., Vasquez, E., & Wienke, W. (2016).
The impact of simulated interviews for Correspondence concerning this article should be
individuals with intellectual disability. Educa- addressed to Rebecca R. Kammes, Department of
tional Technology & Society, 19, 76–88. Counseling, Educational Psychology & Special
Wallerstein, N., & Duran, B. (2010). Community- Education, Michigan State University, 620 Farm
based participatory research contributions to Lane, Room 176, East Lansing, MI, 48824 (e-mail:
intervention research: The intersection of rkammes@msu.edu).
16 Sexuality Questions of Adults With IDD
View publication stats
You might also like
- Casual Sex AgreementDocument5 pagesCasual Sex Agreementpingavin84% (19)
- AdolescenceDocument609 pagesAdolescenceSzabó Dominik100% (7)
- Sexual AstrologyDocument4 pagesSexual AstrologyNordin Yunus50% (2)
- PRECEDE-PROCEED Health Promotion Program Planning ModelDocument18 pagesPRECEDE-PROCEED Health Promotion Program Planning ModelLudwig GeoffreyNo ratings yet
- The Impact of Social Media Powerpoint PresentationDocument36 pagesThe Impact of Social Media Powerpoint PresentationCamille Pineda60% (5)
- Predictors of Access To Sex Education For Children With Intellectual Disabilities in Public SchoolsDocument14 pagesPredictors of Access To Sex Education For Children With Intellectual Disabilities in Public SchoolsHamza HaiderNo ratings yet
- Chapter 2 - Group 4-12humss4Document10 pagesChapter 2 - Group 4-12humss4Angel Jelyn EstrellaNo ratings yet
- Computers in Human Behavior: Celia B. Fisher, Xiangyu Tao, Madeline FordDocument8 pagesComputers in Human Behavior: Celia B. Fisher, Xiangyu Tao, Madeline Fordjennydoan2000No ratings yet
- Analysis of Parental Involvement and Self-Esteem On Secondary School Students in Kieni West Sub-County, Nyeri County, KenyaDocument17 pagesAnalysis of Parental Involvement and Self-Esteem On Secondary School Students in Kieni West Sub-County, Nyeri County, KenyadsfsdgfdgfdgNo ratings yet
- Article Info BackgroundDocument10 pagesArticle Info BackgroundKrishna SharmaNo ratings yet
- Factors Affecting The Level of Awareness On Sex Education of Grade 12 S.Y. 2022-2023 at San Guillermo National HighschoolDocument15 pagesFactors Affecting The Level of Awareness On Sex Education of Grade 12 S.Y. 2022-2023 at San Guillermo National HighschoolDrex RagadioNo ratings yet
- Computers in Human Behavior: Brendan Dempsey, Kathy Looney, Roisin Mcnamara, Sarah Michalek, Eilis HennessyDocument9 pagesComputers in Human Behavior: Brendan Dempsey, Kathy Looney, Roisin Mcnamara, Sarah Michalek, Eilis HennessyFulaneto AltoNo ratings yet
- Research Intellect Disabil - 2019 - Lindahl - Domains of Planning For Future Long Term Care of Adults With Intellectual andDocument13 pagesResearch Intellect Disabil - 2019 - Lindahl - Domains of Planning For Future Long Term Care of Adults With Intellectual andadek wahyuNo ratings yet
- Closer Look On The Plights of The Parentless College Students: A Convergent Parallel AnalysisDocument18 pagesCloser Look On The Plights of The Parentless College Students: A Convergent Parallel AnalysisPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Diverse Disabilities and Dating OnlineDocument21 pagesDiverse Disabilities and Dating OnlineMunadiraNo ratings yet
- A Media Literacy Education Approach To High School Sexual Health Education Immediate Effects of Media Aware On Adolescents Media Sexual Health and Communication Outcomes 2022 SpringerDocument16 pagesA Media Literacy Education Approach To High School Sexual Health Education Immediate Effects of Media Aware On Adolescents Media Sexual Health and Communication Outcomes 2022 SpringerpferradaNo ratings yet
- Oamjms 9e 324Document4 pagesOamjms 9e 324Randy RefnandesNo ratings yet
- Racial and Ethnic Disparities in Childrens Social CareDocument23 pagesRacial and Ethnic Disparities in Childrens Social CareNeil ShellardNo ratings yet
- 1 s2.0 S2667321523000070 MainDocument9 pages1 s2.0 S2667321523000070 Maincristinagalvan.psicologiaNo ratings yet
- Policy AnalysisDocument9 pagesPolicy Analysisapi-567836834No ratings yet
- How Do Gender Stereotypes Affect Children's DevelopmentDocument6 pagesHow Do Gender Stereotypes Affect Children's DevelopmentNguyen Doan Thanh HaNo ratings yet
- The Importance of Sexuality EdDocument9 pagesThe Importance of Sexuality EdAsish DasNo ratings yet
- Exploring Psychosocial Family Issue Related High Risk Sex Involvement Among Female AdolescentsDocument17 pagesExploring Psychosocial Family Issue Related High Risk Sex Involvement Among Female AdolescentsIsabella LantiguaNo ratings yet
- The Challenges Faced by Teachers in Teaching Sex Education in Secondary Schools in Awgu Local Government Area of Enugu StateDocument55 pagesThe Challenges Faced by Teachers in Teaching Sex Education in Secondary Schools in Awgu Local Government Area of Enugu StateNwigwe Promise ChukwuebukaNo ratings yet
- Sexuality in People With Intellectual DisabilityDocument18 pagesSexuality in People With Intellectual DisabilityAlbaNo ratings yet
- Paper - Estabillo 2022Document11 pagesPaper - Estabillo 2022Carito Mical Salazar CarrascoNo ratings yet
- Sex Education and Family BackgroundDocument29 pagesSex Education and Family Backgroundkimb baturianoNo ratings yet
- Zhao 2023-12Document15 pagesZhao 2023-12mahsaNo ratings yet
- Awareness of Secondary School Students Towards Sex EducationDocument8 pagesAwareness of Secondary School Students Towards Sex EducationJulianna Tamayo - AcedoNo ratings yet
- Wurtele Kenny CHD2011Document25 pagesWurtele Kenny CHD2011Chandan MNo ratings yet
- UMAK Employees' Involvement On GAD Mandates and Policies: Inputs To Institutional ResponsivenessDocument9 pagesUMAK Employees' Involvement On GAD Mandates and Policies: Inputs To Institutional ResponsivenessPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Effectiveness of Expressive Art TherapyDocument9 pagesEffectiveness of Expressive Art TherapyTc 04No ratings yet
- Jurnal Kesehatan: Pola Asuh Dan Tipe Keluarga Dengan Perilaku Seks Bebas Pada RemajaDocument8 pagesJurnal Kesehatan: Pola Asuh Dan Tipe Keluarga Dengan Perilaku Seks Bebas Pada RemajaAfifah Az-ZahraNo ratings yet
- Research Template - HUMSSDocument15 pagesResearch Template - HUMSSmay may abelleraNo ratings yet
- Qualitative Sample No. 1Document54 pagesQualitative Sample No. 1Justin MonoyNo ratings yet
- What Do 3 6-Year-Old Children in Finland Know About Sexuality A Child Interview Study in Early EducationDocument21 pagesWhat Do 3 6-Year-Old Children in Finland Know About Sexuality A Child Interview Study in Early Educationiis.afriyanti26No ratings yet
- Copy-Chapter 2 RRLDocument17 pagesCopy-Chapter 2 RRLKlare MoaNo ratings yet
- JPC 13023Document6 pagesJPC 13023arefe samadiNo ratings yet
- Social Challenges of AdolescentDocument13 pagesSocial Challenges of AdolescentsujeetNo ratings yet
- Intellectual Disabilities Paper FinalDocument13 pagesIntellectual Disabilities Paper Finalapi-453017846No ratings yet
- A Systematic Review of Cognitive Functioning Among Young People Who Have Experienced Homelessness Foster Care or PovertyDocument29 pagesA Systematic Review of Cognitive Functioning Among Young People Who Have Experienced Homelessness Foster Care or PovertypaolaNo ratings yet
- Methodology As Pedagogy Trans Lives Social ScienceDocument8 pagesMethodology As Pedagogy Trans Lives Social ScienceEugenia CabralNo ratings yet
- Pemahaman Gender Siswa SDN 2 Wirasaba Kabupaten Purbalingga Di Era Digitalisasi Oleh: Amalia Nur Ramadhani - F2B021007Document12 pagesPemahaman Gender Siswa SDN 2 Wirasaba Kabupaten Purbalingga Di Era Digitalisasi Oleh: Amalia Nur Ramadhani - F2B021007Aditya M WijanarkoNo ratings yet
- Parenting Style, Personality Traits, and Interpersonal Relationships: A Model of Prediction of Internet AddictionDocument23 pagesParenting Style, Personality Traits, and Interpersonal Relationships: A Model of Prediction of Internet AddictionShamså KånwalNo ratings yet
- Literature MatrixDocument4 pagesLiterature MatrixgapangdaisyNo ratings yet
- An Analysis of Students' Perception of Sex Education Programmes and Their Effects On Adolescent Sexual Behaviour in KNUST Junior High School, KumasiDocument15 pagesAn Analysis of Students' Perception of Sex Education Programmes and Their Effects On Adolescent Sexual Behaviour in KNUST Junior High School, KumasiPidot Bryan N.No ratings yet
- Tomenyetal.2017 RIDD PreprintDocument35 pagesTomenyetal.2017 RIDD Preprintsanskriti gautamNo ratings yet
- Sex Education Should Be Taught in Schools VFDocument12 pagesSex Education Should Be Taught in Schools VFEstrella QuinonezNo ratings yet
- EJ1378798Document17 pagesEJ1378798Karen VillanuevaNo ratings yet
- MODULE 5 - Reproductive Health, Issues and ConcernsDocument29 pagesMODULE 5 - Reproductive Health, Issues and ConcernsBryan EduardoNo ratings yet
- Semi Final Group 11Document47 pagesSemi Final Group 11Belza, John Daniel P.No ratings yet
- Research Proposal - ProjectDocument12 pagesResearch Proposal - Projectapi-457299309No ratings yet
- Vass 2022 The-ambivalent-visit-Children-s-experiences-of-relating-with-their-fathersDocument10 pagesVass 2022 The-ambivalent-visit-Children-s-experiences-of-relating-with-their-fathersJu LhyNo ratings yet
- Real-World Connection PaperDocument5 pagesReal-World Connection PaperjobNo ratings yet
- Psy 222 Psych Prob of Mod Youth EssayDocument4 pagesPsy 222 Psych Prob of Mod Youth Essayapi-713298082No ratings yet
- Improving Social Skills in Adolescents and Adults With Autism and Severe To Profound Intellectual Disability: A Review of The LiteratureDocument22 pagesImproving Social Skills in Adolescents and Adults With Autism and Severe To Profound Intellectual Disability: A Review of The LiteratureMacarenaNo ratings yet
- Levels, Trends and Differentials of Teenage Childbearing in IndiaDocument17 pagesLevels, Trends and Differentials of Teenage Childbearing in IndiaThangpi NaulakNo ratings yet
- Adolescent and Family DevelopmentDocument21 pagesAdolescent and Family DevelopmentMatthew LawingNo ratings yet
- Difficult Citizenship': The Precarious Relationships Between Childhood, Sexuality and Access To KnowledgeDocument20 pagesDifficult Citizenship': The Precarious Relationships Between Childhood, Sexuality and Access To KnowledgeLisa RucquoiNo ratings yet
- Factors That Influence Decision-Making Among YouthDocument10 pagesFactors That Influence Decision-Making Among YouthNOR FARHANAH SHAHROOMNo ratings yet
- Sexualization of Children or Human Rights Attitudes Toward Addressing Sexual Orientation Diversity in SchoolDocument33 pagesSexualization of Children or Human Rights Attitudes Toward Addressing Sexual Orientation Diversity in SchoolTamara De Souza CamposNo ratings yet
- Marsack TopolewskiDocument16 pagesMarsack TopolewskiJG Du PlessisNo ratings yet
- Perception On The Role of Parenting Style On Juvenile Delinquency Among Adolescents in The Government Remand Homes Lagos State NigeriaDocument18 pagesPerception On The Role of Parenting Style On Juvenile Delinquency Among Adolescents in The Government Remand Homes Lagos State NigeriaAstin AstinNo ratings yet
- SEXUAL BELIEF CHAPTER ONE and 2 11001Document33 pagesSEXUAL BELIEF CHAPTER ONE and 2 11001Jason CruzNo ratings yet
- Application of The Functional, Expressive and Aesthetic Consumer Needs Model Assessing The Clothing Needs of Adolescent Girls With DisabilitiesDocument10 pagesApplication of The Functional, Expressive and Aesthetic Consumer Needs Model Assessing The Clothing Needs of Adolescent Girls With DisabilitiesAsish DasNo ratings yet
- The Contribution of ADHD and ADocument6 pagesThe Contribution of ADHD and AAsish DasNo ratings yet
- Transgender Experiences of Occupation and The Environment A Scoping ReviewDocument16 pagesTransgender Experiences of Occupation and The Environment A Scoping ReviewAsish DasNo ratings yet
- Why Has So Little Progress BeeDocument6 pagesWhy Has So Little Progress BeeAsish DasNo ratings yet
- Why Has So Little Progress BeeDocument6 pagesWhy Has So Little Progress BeeAsish DasNo ratings yet
- Why Sexuality Education For People With Developmental Disabilities Is So Important - NESCADocument4 pagesWhy Sexuality Education For People With Developmental Disabilities Is So Important - NESCAAsish DasNo ratings yet
- AdolescenceDocument6 pagesAdolescenceAsish DasNo ratings yet
- Acharya 2014 Preparing For Motherhood A Role ForDocument3 pagesAcharya 2014 Preparing For Motherhood A Role ForAsish DasNo ratings yet
- 12 AbstractDocument2 pages12 AbstractAsish DasNo ratings yet
- Fredriksen Goldsen 2012 Disability Among Lesbian Gay and BiDocument6 pagesFredriksen Goldsen 2012 Disability Among Lesbian Gay and BiAsish DasNo ratings yet
- SEXOLOGYDocument144 pagesSEXOLOGYBenny Kofi EffisahNo ratings yet
- Alpha Male State of Mind PDFDocument12 pagesAlpha Male State of Mind PDFRideIT0% (1)
- People Vs CaoileDocument8 pagesPeople Vs CaoileLou StellarNo ratings yet
- 5 Erotic Blueprints Elizabeth CarringtonDocument3 pages5 Erotic Blueprints Elizabeth CarringtonPity UraldeNo ratings yet
- Personal Path To PregnancyDocument62 pagesPersonal Path To PregnancyAna Jane Chua-BitorNo ratings yet
- Nursing Diagnosis - Saliva Test For HIVDocument3 pagesNursing Diagnosis - Saliva Test For HIVMarsha AngelieNo ratings yet
- Tugas Bahasa Inggris Kel 3Document13 pagesTugas Bahasa Inggris Kel 3NopitaNo ratings yet
- Brothels, Baths and Babes Prostitution in The Byzantine Holy LandDocument12 pagesBrothels, Baths and Babes Prostitution in The Byzantine Holy LandOzan BalkanNo ratings yet
- The Sexual SelfDocument30 pagesThe Sexual SelfGilbert BelmisNo ratings yet
- Q4 HEALTH 9 Week 1Document4 pagesQ4 HEALTH 9 Week 1Daphne Gesto SiaresNo ratings yet
- Ancient Primer For Practical Godhead: The Deer Exercise For MenDocument40 pagesAncient Primer For Practical Godhead: The Deer Exercise For MenAnirudhNo ratings yet
- Live Life, Stay Safe (Choral Speaking)Document2 pagesLive Life, Stay Safe (Choral Speaking)Arlynne ZainalNo ratings yet
- Sexuality The Sexual Culture Developing A Sexual Identity AND Risk Factors in Adolescent SexualityDocument15 pagesSexuality The Sexual Culture Developing A Sexual Identity AND Risk Factors in Adolescent SexualityMaybelyn OczonNo ratings yet
- Medical Books GeneralDocument171 pagesMedical Books GeneralJunaidNo ratings yet
- RESEARCH CHAPTER 1 AND 2 FinalDocument36 pagesRESEARCH CHAPTER 1 AND 2 Finaliamthesally yangco100% (1)
- K 2 May 12Document24 pagesK 2 May 12dreamlandbhutanNo ratings yet
- Rape As A Social ProblemDocument11 pagesRape As A Social ProblemOladipo Chukwudi OluwaseunNo ratings yet
- Film Follies, Inc. v. Harl Haas, Etc., 426 U.S. 913 (1976)Document3 pagesFilm Follies, Inc. v. Harl Haas, Etc., 426 U.S. 913 (1976)Scribd Government DocsNo ratings yet
- Young Talk, August 2008Document4 pagesYoung Talk, August 2008Straight Talk FoundationNo ratings yet
- Angles Jeffrey MatthewDocument417 pagesAngles Jeffrey MatthewG. Gordon LiddyNo ratings yet
- GOODSEX - NotesDocument12 pagesGOODSEX - NotesShane BengryNo ratings yet
- ZXXXXDocument2 pagesZXXXXShawn GonzalesNo ratings yet
- Section 375 Penal CodeDocument57 pagesSection 375 Penal CodeAmani NasuhaNo ratings yet
- Arh Powerpoint Pres.Document42 pagesArh Powerpoint Pres.Marissa Fontanil100% (4)
- Graduation Ceremony ScriptDocument109 pagesGraduation Ceremony ScriptJuneilEchavezTecalaNo ratings yet