You might also like
- Focus Smart Plus Science Textbook M2 NPDocument180 pagesFocus Smart Plus Science Textbook M2 NPMichael Galario56% (9)
- Anatomy of Voice: How to Enhance and Project Your Best VoiceFrom EverandAnatomy of Voice: How to Enhance and Project Your Best VoiceRating: 4 out of 5 stars4/5 (3)
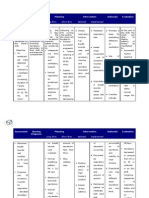
- Nursing Care Plan For Ineffective Airway ClearanceDocument7 pagesNursing Care Plan For Ineffective Airway Clearancearlee marquez96% (118)
- Asthma Nursing Care Plan - NCP - Ineffective Airway ClearanceDocument2 pagesAsthma Nursing Care Plan - NCP - Ineffective Airway ClearanceCyrus De Asis92% (25)
- Sci Focus 2 HB AnswersDocument38 pagesSci Focus 2 HB Answersal83rt777760% (5)
- NCP For AnaphylacticDocument3 pagesNCP For AnaphylacticRommar Romero67% (3)
- Physiological Changes in Elderly RespiDocument23 pagesPhysiological Changes in Elderly RespiIrwan M. IskoberNo ratings yet
- 聲音研究Document54 pages聲音研究roselee0214No ratings yet
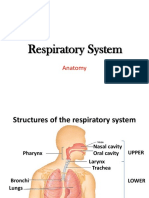
- RespiratoryanatomyDocument5 pagesRespiratoryanatomyMary♡No ratings yet
- NURS1108 Lecture 14 - Respiratory System PART 1 of 2Document62 pagesNURS1108 Lecture 14 - Respiratory System PART 1 of 2Jacia’s SpaceshipNo ratings yet
- Respiratory SystemDocument32 pagesRespiratory SystemJ JamNo ratings yet
- 6 - Respiratory SystemDocument16 pages6 - Respiratory SystemB AuNo ratings yet
- Upper Respiratory Tract AnatomyDocument36 pagesUpper Respiratory Tract AnatomyNatalie HuiNo ratings yet
- Chapter 15 Respiratory SystemDocument3 pagesChapter 15 Respiratory SystemRayumaaa100% (1)
- Chapter 22 Respiratory System AnatomyDocument62 pagesChapter 22 Respiratory System Anatomyamy52891No ratings yet
- The Human Respiratory SystemDocument83 pagesThe Human Respiratory SystemLia lylNo ratings yet
- C-7 Resperatory System (Tu)Document81 pagesC-7 Resperatory System (Tu)Harsh PatelNo ratings yet
- 1.11 ANATOMY - The Nose and Paransal SinusesDocument4 pages1.11 ANATOMY - The Nose and Paransal SinusesPaolo NaguitNo ratings yet
- Sistem Respirasi Stikes WN PDFDocument107 pagesSistem Respirasi Stikes WN PDFEkafatikasariNo ratings yet
- A.S.a Chapter 12 - The Respiratory SystemDocument8 pagesA.S.a Chapter 12 - The Respiratory Systemkoshiaiko21No ratings yet
- Functional Anatomy of The Respiratory System 2. Respiratory PhysiologyDocument62 pagesFunctional Anatomy of The Respiratory System 2. Respiratory PhysiologySara ANo ratings yet
- 2 - Respiratory SystemDocument9 pages2 - Respiratory SystemHannah Grace CorveraNo ratings yet
- Respiratory SystemDocument7 pagesRespiratory SystemRichard Castada Guanzon Jr.No ratings yet
- Jurnal Anatomi IDocument20 pagesJurnal Anatomi IStanislaus Stanley SuhermanNo ratings yet
- Micro - Respiratory SystemDocument3 pagesMicro - Respiratory SystemKaren ValdezNo ratings yet
- Lung Anatomy and Airflow ReportDocument11 pagesLung Anatomy and Airflow Reporttshireletso “TROY” nkunaNo ratings yet
- The Respiratory System: A Fixed Learning ModuleDocument38 pagesThe Respiratory System: A Fixed Learning ModulerezaNo ratings yet
- Chapter 6 Respiratory SystemDocument70 pagesChapter 6 Respiratory SystemWenzy Razzie cruzNo ratings yet
- BI 233 Lab 17Document11 pagesBI 233 Lab 17Cj LinceNo ratings yet
- Respiratory SystemDocument25 pagesRespiratory Systemlobna HijliNo ratings yet
- 2 - Respiratory SystemDocument9 pages2 - Respiratory SystemHannah Grace CorveraNo ratings yet
- Respiratory System Anatomy: Pre-Lab ExercisesDocument12 pagesRespiratory System Anatomy: Pre-Lab ExercisesAisha MagarangNo ratings yet
- Respiratory SystemDocument89 pagesRespiratory SystemSuzuke Mae Nijo100% (1)
- Respiratory System ReviewerDocument7 pagesRespiratory System ReviewerVictoria Ellex TiomicoNo ratings yet
- Respiratory System Cut and Paste AnswersDocument1 pageRespiratory System Cut and Paste AnswersLayal GhaddarNo ratings yet
- 11 Nasal Cavity and Paranasal Sinuses-Dr - GosaiDocument41 pages11 Nasal Cavity and Paranasal Sinuses-Dr - GosaiDr.B.B.GosaiNo ratings yet
- מצגת 8Document37 pagesמצגת 8משתמשת משתשמתNo ratings yet
- External Respiration: Angiotensin-Converting EnzymeDocument4 pagesExternal Respiration: Angiotensin-Converting EnzymeEllä PabustanNo ratings yet
- Respiratory SystemDocument13 pagesRespiratory SystemAly HannahNo ratings yet
- Anatomy Final pt.2Document8 pagesAnatomy Final pt.2Gladys Mae S. BañesNo ratings yet
- Practical Unit 5 PDFDocument10 pagesPractical Unit 5 PDFSanndy milesNo ratings yet
- CH 23 Respiration F 2017 SRMDocument153 pagesCH 23 Respiration F 2017 SRMJuliaNo ratings yet
- Respiratory SystemDocument12 pagesRespiratory SystemCUESCANO, CRISTEL G. BSMT 2-ANo ratings yet
- Pre-Finals Topic 1 AnaphyDocument5 pagesPre-Finals Topic 1 AnaphyGlenice Joy SenocNo ratings yet
- Practical Unit 10 Done PDFDocument10 pagesPractical Unit 10 Done PDFSanndy milesNo ratings yet
- Gas Exchange ActivityDocument3 pagesGas Exchange ActivitySophie BaromanNo ratings yet
- O CO O CO O CO: Chapter 15: Respiratory SystemDocument3 pagesO CO O CO O CO: Chapter 15: Respiratory SystemPrecious Faith RodriguezNo ratings yet
- Anatomy CHP 13 NotesDocument5 pagesAnatomy CHP 13 NotesIsland RaeNo ratings yet
- 12 Respiratory System - ATFDocument43 pages12 Respiratory System - ATFLucas BarbosaNo ratings yet
- Parts of The Respiratory System & Their FunctionsDocument38 pagesParts of The Respiratory System & Their FunctionsSaajid AmraNo ratings yet
- The Respiratory System Lec TransesDocument10 pagesThe Respiratory System Lec TransesVENUS LIRIA PANTINo ratings yet
- 1 - Upper Respiratory TractDocument12 pages1 - Upper Respiratory TractAbdiwahab AbdirasakNo ratings yet
- Respiratory Disorders (Completed)Document55 pagesRespiratory Disorders (Completed)Czejan Rae TabaranzaNo ratings yet
- 11j Caybot Jashjovian Task11Document19 pages11j Caybot Jashjovian Task11Wonder Selene RouxNo ratings yet
- Lab CH36Document4 pagesLab CH36Gricelda VasquezNo ratings yet
- The Respiratory SystemDocument10 pagesThe Respiratory SystemMiguel GumatayNo ratings yet
- WK 4 Respiratory 2023Document38 pagesWK 4 Respiratory 2023Basmala HebaNo ratings yet
- Respiratory SystemDocument9 pagesRespiratory SystemYesha Del RosarioNo ratings yet
- Anatomy, Histology and Physiology-Biochemistry of The Respiratory SystemDocument81 pagesAnatomy, Histology and Physiology-Biochemistry of The Respiratory SystemEldhaNo ratings yet
- 36 AnswerDocument7 pages36 AnswerJasmine Nicole EnriquezNo ratings yet
- Edited - Structures of The Upper Respiratory TractDocument1 pageEdited - Structures of The Upper Respiratory Tractwk79wx84ryNo ratings yet
- Captions&Slides MergedDocument83 pagesCaptions&Slides Mergedstudent4007No ratings yet
- Respiratory System: Joanna Cabuhay 293 Calingacion ST - Poblacion SibulanDocument6 pagesRespiratory System: Joanna Cabuhay 293 Calingacion ST - Poblacion SibulanJoanna :DNo ratings yet
- Respiratory System Function - Respiratory Organs: Structure and FunctionDocument4 pagesRespiratory System Function - Respiratory Organs: Structure and Functionvinnie0905No ratings yet
- Deep Breathing Exercises: Procedure AssessmentDocument3 pagesDeep Breathing Exercises: Procedure AssessmentJelly Jia100% (1)
- PB 1 - NP 3 (Final)Document18 pagesPB 1 - NP 3 (Final)AnnizaNo ratings yet
- Sci9 Q1 Mod2 Effects of Lifestyle On The Respiratory and Circulatory Systems Version3 Edited3Document23 pagesSci9 Q1 Mod2 Effects of Lifestyle On The Respiratory and Circulatory Systems Version3 Edited3NOVA LESLIE AGAPAYNo ratings yet
- Assessment of Patients With Respiratory Disorders Basic Respiratory Care ModalitiesDocument15 pagesAssessment of Patients With Respiratory Disorders Basic Respiratory Care ModalitiesJhosita Flora LarocoNo ratings yet
- ICD10WHO2007 TnI4Document1,656 pagesICD10WHO2007 TnI4Kanok SongprapaiNo ratings yet
- Bronchial Asthma - HandoutDocument3 pagesBronchial Asthma - HandoutkimerellaNo ratings yet
- Hypernatremia Hyperkalemia: of Increased Serum K+Document3 pagesHypernatremia Hyperkalemia: of Increased Serum K+edited_chenNo ratings yet
- Community Acquired PneumoniaDocument7 pagesCommunity Acquired PneumoniaJoshuaOng100% (1)
- 2Document78 pages2api-3744136No ratings yet
- Case Study of PNEUMONIADocument19 pagesCase Study of PNEUMONIAcarls burg a. resurreccion78% (9)
- Physiological Basis of Respiratory Disease (Qutayba Hamid, Joanne Shannon MD, James Martin)Document816 pagesPhysiological Basis of Respiratory Disease (Qutayba Hamid, Joanne Shannon MD, James Martin)RLibdehNo ratings yet
- NCM 112 Care of Clients With Problems in Oxygenation, Fluid and Electrolytes, Infectious, Inflammatory & Immunologic ReactionDocument52 pagesNCM 112 Care of Clients With Problems in Oxygenation, Fluid and Electrolytes, Infectious, Inflammatory & Immunologic ReactionJIMENEZ, TRISHA MARIE D.100% (1)
- IGC2 Elem 6 (Chemical and Biological Health Hazard Control)Document77 pagesIGC2 Elem 6 (Chemical and Biological Health Hazard Control)jimboy37875% (4)
- StridorDocument20 pagesStridortkeat_9No ratings yet
- Case Presentation in Geriatric Ward "Cancer of The Larynx"Document130 pagesCase Presentation in Geriatric Ward "Cancer of The Larynx"Christina GutierrezNo ratings yet
- Smoke Inhalation: Smoke Inhalation Is The Breathing in of Harmful FumesDocument4 pagesSmoke Inhalation: Smoke Inhalation Is The Breathing in of Harmful FumesalanNo ratings yet
- ANATOMY Study Lower Respiratory TractDocument3 pagesANATOMY Study Lower Respiratory TractLP BenozaNo ratings yet
- What Do The Lungs Do, and How Do They Function?: StructureDocument15 pagesWhat Do The Lungs Do, and How Do They Function?: StructurethenameisvijayNo ratings yet
- 4 231019120736 607a0a70Document51 pages4 231019120736 607a0a70ASHISH KANYALNo ratings yet
- Ch13 Respiratory PresentationDocument90 pagesCh13 Respiratory Presentationmedic99No ratings yet
- Respiratory AssessmentDocument38 pagesRespiratory AssessmentNisha MwlzNo ratings yet
- Pharmacology McqsDocument7 pagesPharmacology McqsAshraf AboNo ratings yet
- Complete Guide To Homeopathy MM Drug PictureDocument40 pagesComplete Guide To Homeopathy MM Drug Picturerumana.kulsum43No ratings yet
- NCM 112 Lecture NotesDocument5 pagesNCM 112 Lecture NotesSureen RegularNo ratings yet