You might also like
- W@H PermitDocument2 pagesW@H PermitJixtha SaintNo ratings yet
- Risk Assess JSA Bolt Tightening 012Document7 pagesRisk Assess JSA Bolt Tightening 012Abdeldjalil Ferhati100% (2)
- Main Contractor - Larsen and Toubro Limited Sub Contractor - Danway EMEDocument7 pagesMain Contractor - Larsen and Toubro Limited Sub Contractor - Danway EMERoshan de SilvaNo ratings yet
- JHA ConcretingDocument3 pagesJHA Concretingfatimah beluhi75% (4)
- JSA 115 Slip New Drill-Line On BlocksDocument4 pagesJSA 115 Slip New Drill-Line On BlocksanhlhNo ratings yet
- Is Valid Only With Original Photo ID: Railway Recruitment BoardDocument3 pagesIs Valid Only With Original Photo ID: Railway Recruitment BoardNirajan MarwaitNo ratings yet
- Oil Circulation Tank 674 GB Register 7Document6 pagesOil Circulation Tank 674 GB Register 7hendraNo ratings yet
- VPO - SAFE.3.1.07.05. Energized Electrical Works PermitDocument8 pagesVPO - SAFE.3.1.07.05. Energized Electrical Works PermitsisocaylNo ratings yet
- JSA FormDocument4 pagesJSA Formandrew rachmanNo ratings yet
- CHSEMS-PPE RequirementDocument4 pagesCHSEMS-PPE RequirementHSE BalinusraNo ratings yet
- Job Safety Analysis Form: CSCCB Hole WatchDocument4 pagesJob Safety Analysis Form: CSCCB Hole WatchFrank ElizardoNo ratings yet
- Appendix 6 - HR WAH REV 2-Restrict EditingDocument4 pagesAppendix 6 - HR WAH REV 2-Restrict Editingamri ashaariNo ratings yet
- Air Conditioner InstallationDocument3 pagesAir Conditioner InstallationWalid KhelfaNo ratings yet
- TRA Renovation, Service For Building and Office Construction (Ex Telkom Building) Rev1Document8 pagesTRA Renovation, Service For Building and Office Construction (Ex Telkom Building) Rev1Dol29No ratings yet
- JSA - Blooming Mill T-U-V Bay Axis 42 To 48Document6 pagesJSA - Blooming Mill T-U-V Bay Axis 42 To 48mohanNo ratings yet
- 14 Working at Height - Ra - JSA - R1Document1 page14 Working at Height - Ra - JSA - R1BHARAT TALPADANo ratings yet
- IM-08-B HSE Wall Grinding For Finishing WorkDocument2 pagesIM-08-B HSE Wall Grinding For Finishing WorkAnsari HarisNo ratings yet
- Connexion de Cable MT Avec Boite JonctionDocument3 pagesConnexion de Cable MT Avec Boite JonctionWalid KhelfaNo ratings yet
- Electrical InstallationDocument3 pagesElectrical InstallationWalid KhelfaNo ratings yet
- JSA Loading & UnloadingDocument2 pagesJSA Loading & UnloadingSodikinNo ratings yet
- JSA - Low Voltage PanelDocument19 pagesJSA - Low Voltage PanelASLAM MULANINo ratings yet
- Proper Communication Should Be Done During Working While Using 2 or More Chain Block - Work Must Be Done With Proper SupervisionDocument2 pagesProper Communication Should Be Done During Working While Using 2 or More Chain Block - Work Must Be Done With Proper SupervisionDautsons InfratechNo ratings yet
- Fall Hazard Assessment Form 0Document5 pagesFall Hazard Assessment Form 0Waqas KhanNo ratings yet
- Hot Work Permit Example 02Document2 pagesHot Work Permit Example 02Marjan BrčićNo ratings yet
- Biopolis TBM 17 Feb 2024Document3 pagesBiopolis TBM 17 Feb 2024SelvamNo ratings yet
- HOT WORK - SILOS - Tesarski Radovi - 23.02.2022.Document2 pagesHOT WORK - SILOS - Tesarski Radovi - 23.02.2022.Marin MileticNo ratings yet
- PTW S13 310523Document2 pagesPTW S13 310523letslearnbd01No ratings yet
- Job Safety Analysis: Required References Jsa ReviewDocument3 pagesJob Safety Analysis: Required References Jsa ReviewWalid KhelfaNo ratings yet
- Job Safety Analysis: Required References Jsa ReviewDocument3 pagesJob Safety Analysis: Required References Jsa ReviewWalid KhelfaNo ratings yet
- Safety JSA Workin at HeightDocument1 pageSafety JSA Workin at HeightBHARAT TALPADANo ratings yet
- Scaffolding CertificatesDocument1 pageScaffolding CertificatesRAZANo ratings yet
- Job Safety Analysis: Required References Jsa ReviewDocument3 pagesJob Safety Analysis: Required References Jsa ReviewWalid KhelfaNo ratings yet
- JSA Hot WorkDocument1 pageJSA Hot WorkAli Ramadhan AksodiNo ratings yet
- Mosca Point of Work Risk AssessmentDocument1 pageMosca Point of Work Risk AssessmentBryanNo ratings yet
- Lifting Work PermitDocument1 pageLifting Work PermitRadha BuildtechNo ratings yet
- Directions For Completing Confined Space Permit Work DescriptionDocument11 pagesDirections For Completing Confined Space Permit Work DescriptionMOHAMEDNo ratings yet
- 003 ABGJHA003 Lifting and Placement of Cabins and ContainersDocument2 pages003 ABGJHA003 Lifting and Placement of Cabins and ContainersALBILAL HSENo ratings yet
- Tous Travaux D'entretien, de Remplacement de Pièces Mécaniques, Hydrauliques, Pneumatiques Et Électriques Et de SoudureDocument5 pagesTous Travaux D'entretien, de Remplacement de Pièces Mécaniques, Hydrauliques, Pneumatiques Et Électriques Et de Soudureloua cece antoineNo ratings yet
- JSA Finishing Temporary FacilitiesDocument6 pagesJSA Finishing Temporary Facilitiesjet Louis Magallones100% (1)
- Ptwno 26: 571al ExpiryDocument2 pagesPtwno 26: 571al Expirysufiyan sskNo ratings yet
- Site Job Safety Analysis (JSA)Document1 pageSite Job Safety Analysis (JSA)Brian TanNo ratings yet
- Jsa Panel SullayilDocument6 pagesJsa Panel SullayilthennarasuNo ratings yet
- Job Safety Analysis: Required References Jsa ReviewDocument5 pagesJob Safety Analysis: Required References Jsa ReviewMoaatazz Nouisri100% (1)
- Height WorkDocument2 pagesHeight WorkDautsons InfratechNo ratings yet
- Hro PTW R1Document1 pageHro PTW R1JISHNU EHSNo ratings yet
- Hazardous Work Permit: The Completion of The Following Work Is AuthorizedDocument3 pagesHazardous Work Permit: The Completion of The Following Work Is AuthorizedМарко ИвановићNo ratings yet
- P111-RSME-TRA-007 - TRA For Cold Tie in PDFDocument4 pagesP111-RSME-TRA-007 - TRA For Cold Tie in PDFDarius DsouzaNo ratings yet
- Riyadh Cargo Terminal Project Zamil SteelDocument41 pagesRiyadh Cargo Terminal Project Zamil SteelGhost RiderNo ratings yet
- Packing Pumps New - FO-GL-HAL-HSE-0103FDocument4 pagesPacking Pumps New - FO-GL-HAL-HSE-0103FMohamed El-SawahNo ratings yet
- JSA - Confined Space - Civil WorksDocument7 pagesJSA - Confined Space - Civil WorksSusil Kumar SahooNo ratings yet
- JSA LandFill KHPT-BBB JODocument1 pageJSA LandFill KHPT-BBB JOICEDA HumNo ratings yet
- Jsa Breaking Down Bop Into Handling SkidDocument4 pagesJsa Breaking Down Bop Into Handling SkidPaulNo ratings yet
- Pre Job Hazard Assessment: Our Goal Is Injuries in The WorkplaceDocument1 pagePre Job Hazard Assessment: Our Goal Is Injuries in The WorkplaceNadya ShintaNo ratings yet
- SWP - 21!06!2019 (Demolish Existing Ceiling & Raised Floor)Document4 pagesSWP - 21!06!2019 (Demolish Existing Ceiling & Raised Floor)Jhon Luther PNo ratings yet
- Job Safety Analysis Record Sheet: Cause & Effect Metrix TestDocument2 pagesJob Safety Analysis Record Sheet: Cause & Effect Metrix TestFernandoMarquezNo ratings yet
- JSA For Oil Pressure For GovernorDocument3 pagesJSA For Oil Pressure For GovernorAkhli RohmatulohNo ratings yet
- P111-Rsme-Tra-007 - Tra For Cold Tie inDocument5 pagesP111-Rsme-Tra-007 - Tra For Cold Tie inDarius DsouzaNo ratings yet
- GE PTW Confined SpacesDocument2 pagesGE PTW Confined SpacesKural MurugesanNo ratings yet
- Jsa MV Cable Pulling, Termination and TestingDocument11 pagesJsa MV Cable Pulling, Termination and TestingMohammad AqilNo ratings yet
- Genie E Series Slab Scissor Lift OperationDocument11 pagesGenie E Series Slab Scissor Lift OperationSanket Arun MoreNo ratings yet
- Genie E Series Slab Scissor Lift Operation PDFDocument11 pagesGenie E Series Slab Scissor Lift Operation PDFRajesh gpNo ratings yet
- Rescue Plan - KM 50+600.Document5 pagesRescue Plan - KM 50+600.rian1099No ratings yet
- The Manila Hotel: Events Set-Up Work PermitDocument1 pageThe Manila Hotel: Events Set-Up Work PermitMadz Alcoy BautistaNo ratings yet
- Ashok Shuttering Measurment: S.NO. Description Nos. Length Breadth Total Oty. RemarksDocument3 pagesAshok Shuttering Measurment: S.NO. Description Nos. Length Breadth Total Oty. RemarksNirajan MarwaitNo ratings yet
- Quotaion For 53Document1 pageQuotaion For 53Nirajan MarwaitNo ratings yet
- Tutorial Material For Mandatory Basic Safety Training Course (Construction Work)Document22 pagesTutorial Material For Mandatory Basic Safety Training Course (Construction Work)Nirajan MarwaitNo ratings yet
- SF 23 & 24 Work Permit Lifting - Tandem LiftingDocument8 pagesSF 23 & 24 Work Permit Lifting - Tandem LiftingNirajan Marwait100% (2)
- Pole in Between CP-55 & P-56: MVR F875Document5 pagesPole in Between CP-55 & P-56: MVR F875Nirajan MarwaitNo ratings yet
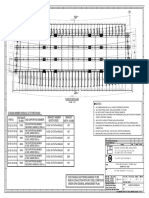
- Notes: - : Plan of Deck SlabDocument1 pageNotes: - : Plan of Deck SlabNirajan MarwaitNo ratings yet
- Risk Assessment For Erection of Steel GirderDocument11 pagesRisk Assessment For Erection of Steel GirderNirajan MarwaitNo ratings yet
- Drain CoverDocument2 pagesDrain CoverNirajan MarwaitNo ratings yet
- HIV PolicyDocument1 pageHIV PolicyNirajan MarwaitNo ratings yet
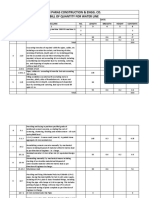
- Jai Paras Construction & Engg. Co. Bill of Quantity For Water LineDocument3 pagesJai Paras Construction & Engg. Co. Bill of Quantity For Water LineNirajan MarwaitNo ratings yet
- Ehs Risk Register / Assessment: Name of The Project Reference No Activities CoveredDocument7 pagesEhs Risk Register / Assessment: Name of The Project Reference No Activities CoveredNirajan MarwaitNo ratings yet
- Jai Paras Construction & Engg. Co. Bill of Quantity For Storm Water LineDocument3 pagesJai Paras Construction & Engg. Co. Bill of Quantity For Storm Water LineNirajan MarwaitNo ratings yet
- Particulars QTY Unit Rate Amount 1 2 3 4 5: S.No Ref. NoDocument1 pageParticulars QTY Unit Rate Amount 1 2 3 4 5: S.No Ref. NoNirajan MarwaitNo ratings yet
- PIONEER Fabricators (P) LTD.: AN ISO 9001:2008 COMPANYDocument1 pagePIONEER Fabricators (P) LTD.: AN ISO 9001:2008 COMPANYNirajan MarwaitNo ratings yet
- Qap PDFDocument11 pagesQap PDFNirajan MarwaitNo ratings yet
- Monthly Progress ReportDocument8 pagesMonthly Progress ReportNirajan MarwaitNo ratings yet
- Coolingwater 140301175552 Phpapp01Document9 pagesCoolingwater 140301175552 Phpapp01Vasanth Rajan100% (1)
- Usg - 10060456 1.0Document228 pagesUsg - 10060456 1.0sahtekir0% (1)
- How Cement Is MadeDocument2 pagesHow Cement Is MadeJo MNo ratings yet
- Lecture 02 - Microcontroller Core Features and ArchitectureDocument12 pagesLecture 02 - Microcontroller Core Features and ArchitectureAwaisNo ratings yet
- Amr Ashraf Abdallah C.V - MEP CoordinatorDocument4 pagesAmr Ashraf Abdallah C.V - MEP CoordinatorAmr AshrafNo ratings yet
- Understanding of Dynamic Voltage: Restorers Through MATLAB SimulationDocument6 pagesUnderstanding of Dynamic Voltage: Restorers Through MATLAB SimulationPhạm Quý ThắngNo ratings yet
- Sa227 Series: Maintenance ManualDocument28 pagesSa227 Series: Maintenance ManualKIKENo ratings yet
- Shimge Pump-CatalogueDocument19 pagesShimge Pump-CatalogueJulie MahadiNo ratings yet
- DME Unitwise Question BankDocument24 pagesDME Unitwise Question BanksureshkumarNo ratings yet
- Higher or Lower DensityDocument0 pagesHigher or Lower DensitynasirmuzaffarNo ratings yet
- Design Methods For Confined FlowDocument4 pagesDesign Methods For Confined FlowZaid JamilNo ratings yet
- 02 SiteworksDocument49 pages02 SiteworksAdon Dela RosaNo ratings yet
- METAL SOLUTION INDUSTRIES Product CatalogueDocument16 pagesMETAL SOLUTION INDUSTRIES Product CatalogueSaad AkramNo ratings yet
- Jaquar CatalogDocument99 pagesJaquar Catalogjagadeesh_92003No ratings yet
- Control Lab1Document59 pagesControl Lab1Marlon Boucaud0% (1)
- Daewoo RF 420Document33 pagesDaewoo RF 420Adi Antonescu0% (1)
- Acer Aspire 5622Document1 pageAcer Aspire 5622spscribd1-2No ratings yet
- Lithium Ion Battery Labels 3480 - 1Document3 pagesLithium Ion Battery Labels 3480 - 1josephNo ratings yet
- File Encryption System: Bhumit Malvi (Roll No 26) Ved Kokane (Roll No. 20) Vinit More (Roll No. 32)Document11 pagesFile Encryption System: Bhumit Malvi (Roll No 26) Ved Kokane (Roll No. 20) Vinit More (Roll No. 32)Bhumit MalviNo ratings yet
- Visual KVDocument10 pagesVisual KVChong Kean WahNo ratings yet
- Steam Turbine Auxiliaries Question & AnswersDocument10 pagesSteam Turbine Auxiliaries Question & AnswersLaxman Veerepalli100% (1)
- Part No. Description Qty. Part No. Description QtyDocument2 pagesPart No. Description Qty. Part No. Description QtyRiyaz SiddiqueNo ratings yet
- University of Jordan School of Engineering Mechatronics Engineering Department Transducers LaboratoryDocument3 pagesUniversity of Jordan School of Engineering Mechatronics Engineering Department Transducers LaboratoryAbdullah AffanehNo ratings yet
- Technical Drawing And: Computer Aided DesignDocument15 pagesTechnical Drawing And: Computer Aided DesigncatalinNo ratings yet
- PVC Conduit Pipes Manufacturing BusinessDocument70 pagesPVC Conduit Pipes Manufacturing BusinessmmtaassociatesNo ratings yet
- Packers and Movers in DelhiDocument2 pagesPackers and Movers in DelhiPriya GurgNo ratings yet
- Nx4 User ManualDocument24 pagesNx4 User ManualTri BuiNo ratings yet