You might also like
- Human Geography Places and Regions in Global Context PDFDocument8 pagesHuman Geography Places and Regions in Global Context PDFJosh MaiyoNo ratings yet
- Sensory Processing BrochureDocument3 pagesSensory Processing Brochureapi-383884645No ratings yet
- January 2016 - InternationalDocument72 pagesJanuary 2016 - InternationalAlis Pastrana100% (1)
- Disorder: PTSD: Factors: PREDISPOSINGDocument8 pagesDisorder: PTSD: Factors: PREDISPOSINGAldrin PaulinoNo ratings yet
- Disorder: Anorexia & Bulimia Nervosa: Factors: PREDISPOSINGDocument10 pagesDisorder: Anorexia & Bulimia Nervosa: Factors: PREDISPOSINGAldrin PaulinoNo ratings yet
- Biological and Environmental Factors.": Perdev'T ExamDocument1 pageBiological and Environmental Factors.": Perdev'T ExamMikka RoqueNo ratings yet
- Ethics in Psychology Chap 1 ReviewerDocument2 pagesEthics in Psychology Chap 1 ReviewerJermaine Joie GamilNo ratings yet
- Claire Orange PDDocument89 pagesClaire Orange PDmelaniesNo ratings yet
- Pedia G&DDocument2 pagesPedia G&DKim RamosNo ratings yet
- Developmental PsychologyDocument3 pagesDevelopmental Psychology85784703No ratings yet
- INFOGRAPHDocument3 pagesINFOGRAPHJADE PATEGANo ratings yet
- Client Ed TableDocument3 pagesClient Ed Tableirish274No ratings yet
- Ethics Module Lesson4Document8 pagesEthics Module Lesson4Cristine Mae PreguntaNo ratings yet
- Language For StudentsDocument42 pagesLanguage For StudentsaplesgjskNo ratings yet
- FOI Quick ReferenceDocument7 pagesFOI Quick ReferenceBob CurtisNo ratings yet
- Lesson 1 - Theory of Frued, Erickson, Piaget & Kholberg (Personal Development)Document7 pagesLesson 1 - Theory of Frued, Erickson, Piaget & Kholberg (Personal Development)Miracle LakeNo ratings yet
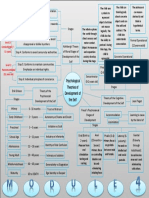
- Psychological Theories of Development of The Self: Level 1: Preconventional (Younger Than 6)Document1 pagePsychological Theories of Development of The Self: Level 1: Preconventional (Younger Than 6)jebzkiah productionNo ratings yet
- Fundamentals of Nursing Lecture1Document6 pagesFundamentals of Nursing Lecture1Kazlle Sheen MinianoNo ratings yet
- 117A-PRELIM-ELEARNING-2nd SemDocument4 pages117A-PRELIM-ELEARNING-2nd SemJovielyn KowetNo ratings yet
- Top Models of Ethical Decision MakingDocument13 pagesTop Models of Ethical Decision MakingDilah AzmanNo ratings yet
- OT Interventions For ASDDocument42 pagesOT Interventions For ASDTitus LeeNo ratings yet
- Rules of BehaviorDocument6 pagesRules of BehaviorGenesis AdcapanNo ratings yet
- Pediatric Nursing Lecture 59 Pages Pg. 274 332Document58 pagesPediatric Nursing Lecture 59 Pages Pg. 274 332ShiraishiNo ratings yet
- Theory Assignment 1Document2 pagesTheory Assignment 1api-322059527No ratings yet
- Freud Kohlberg Erkson Piaget Maslow MRDocument13 pagesFreud Kohlberg Erkson Piaget Maslow MRPrincess Pauline LaizNo ratings yet
- Sarahina CI EDUC2 A2Document8 pagesSarahina CI EDUC2 A2sarahinacamilaNo ratings yet
- NCE Human Growth and Development PDF For Email BackupDocument12 pagesNCE Human Growth and Development PDF For Email BackupAmy D.100% (1)
- FINALS ACTIVITY 1 EDUC 5Document2 pagesFINALS ACTIVITY 1 EDUC 5yuri lloydNo ratings yet
- Go To Page Word 0617022Document18 pagesGo To Page Word 0617022api-618483692No ratings yet
- Promoting Normal Growth and DevelopmentDocument3 pagesPromoting Normal Growth and DevelopmentAlly AngcosNo ratings yet
- HlthEduc Module 2 3Document5 pagesHlthEduc Module 2 3TRISHA KATE MEDINANo ratings yet
- Age GroupDocument5 pagesAge GroupsustiguerchristianpaulNo ratings yet
- PerdevDocument2 pagesPerdevJabi ZorgoNo ratings yet
- Diagnostic Categories-Abnormal PsychDocument16 pagesDiagnostic Categories-Abnormal PsychWarren GreyNo ratings yet
- Pediatric Nursing: Growth, Development and Nursing CareDocument59 pagesPediatric Nursing: Growth, Development and Nursing CareYmon TuallaNo ratings yet
- Nursingprocessandram PDFDocument34 pagesNursingprocessandram PDFvijaykadam_ndaNo ratings yet
- Team Teach TrainingDocument2 pagesTeam Teach TrainingjamilaakhatunnNo ratings yet
- Personal development theories under 40 charactersDocument3 pagesPersonal development theories under 40 charactersCamylia CocjinNo ratings yet
- Go To Page Word 2022Document17 pagesGo To Page Word 2022api-673370235No ratings yet
- Turaray Jonelyn ED 7 Activity 3Document7 pagesTuraray Jonelyn ED 7 Activity 3KyleNo ratings yet
- Autism Spectrum Disorders & Intellectual DisabilityDocument61 pagesAutism Spectrum Disorders & Intellectual Disabilityncastro1319No ratings yet
- Module 8 Moral-DevelopmentDocument8 pagesModule 8 Moral-DevelopmentHimawari Torres100% (1)
- Module 7Document5 pagesModule 7Alex Grace DiagbelNo ratings yet
- Systems Thinking ApproachDocument2 pagesSystems Thinking ApproachDaisy100% (8)
- Human Behavior VictimologyDocument61 pagesHuman Behavior VictimologyRey Mark GedaroNo ratings yet
- Chapter 6 PsychDocument5 pagesChapter 6 PsychGerry Jimenez Sao-anNo ratings yet
- EP-2-Cho-Concept Map-Developmental StagesDocument1 pageEP-2-Cho-Concept Map-Developmental StagesKZHAYRUUNo ratings yet
- Perdev Q3Document5 pagesPerdev Q3Sam VillegasNo ratings yet
- Effective Communication SkillsDocument6 pagesEffective Communication SkillsEricson CandelariaNo ratings yet
- MMBP Mod 7Document32 pagesMMBP Mod 7shaziafirdoosNo ratings yet
- Facilitating Learner-Centered Teaching 1st Sem SummaryDocument3 pagesFacilitating Learner-Centered Teaching 1st Sem Summarygothic wontonNo ratings yet
- Seatwork #1 (Vivas Mariah Jamby A. BSN-I)Document8 pagesSeatwork #1 (Vivas Mariah Jamby A. BSN-I)Jamby VivasNo ratings yet
- IST Module 2 Day 3 Revised HANDOUT Introduction To Modes Saturday October 10thDocument25 pagesIST Module 2 Day 3 Revised HANDOUT Introduction To Modes Saturday October 10thxx xxNo ratings yet
- PED7 Facilitating Learner Centered TeachingDocument11 pagesPED7 Facilitating Learner Centered TeachingGina Liza CanamaNo ratings yet
- Local Media2246351459788256841Document4 pagesLocal Media2246351459788256841Reyster AfricaNo ratings yet
- 4 - Health and Safety Culture.Document18 pages4 - Health and Safety Culture.Aldrien CabinteNo ratings yet
- Facilitating Learning Through Meta-CognitionDocument337 pagesFacilitating Learning Through Meta-CognitionMichelle ArregLado VistalNo ratings yet
- Trauma-Sensitive SEL for Student WellnessDocument45 pagesTrauma-Sensitive SEL for Student Wellnesstri saksonoNo ratings yet
- Biological Risk Factors Symptoms Key FactsDocument2 pagesBiological Risk Factors Symptoms Key FactsKa Chun ChanNo ratings yet
- Module 2 Slides For SharingDocument54 pagesModule 2 Slides For Sharingjonah.momoNo ratings yet
- Abnormal Psychology (Last Discussion)Document18 pagesAbnormal Psychology (Last Discussion)FLORLYN VERALNo ratings yet
- Emotional Intelligence 101: Developing EQ for Success in Life and WorkFrom EverandEmotional Intelligence 101: Developing EQ for Success in Life and WorkNo ratings yet
- Measures of Central Tendency ExplainedDocument4 pagesMeasures of Central Tendency ExplainedAldrin Paulino0% (1)
- Preventing Occupational Exposures To Antineoplastic and Other Hazardous Drugs in Health Care SettingsDocument1 pagePreventing Occupational Exposures To Antineoplastic and Other Hazardous Drugs in Health Care SettingsAldrin PaulinoNo ratings yet
- Guide Questions (NSTP)Document5 pagesGuide Questions (NSTP)Aldrin PaulinoNo ratings yet
- Rationale For Questions 45-48Document1 pageRationale For Questions 45-48Aldrin PaulinoNo ratings yet
- Hazardous Drug Exposures in Health Care (Reaction Paper)Document1 pageHazardous Drug Exposures in Health Care (Reaction Paper)Aldrin PaulinoNo ratings yet
- Meeting Agenda TemplateDocument1 pageMeeting Agenda TemplateAldrin PaulinoNo ratings yet
- My Sister's Keeper-Movie ReflectionDocument1 pageMy Sister's Keeper-Movie ReflectionAldrin PaulinoNo ratings yet
- The 17 Indisputable Laws of TeamworkDocument4 pagesThe 17 Indisputable Laws of TeamworkAldrin PaulinoNo ratings yet
- Instructional Plan (Dengue)Document1 pageInstructional Plan (Dengue)Aldrin PaulinoNo ratings yet
- A. Narrative Evaluation of Actual Nursing ProblemsDocument1 pageA. Narrative Evaluation of Actual Nursing ProblemsAldrin PaulinoNo ratings yet
- Treatment, Diet, (CNP)Document1 pageTreatment, Diet, (CNP)Aldrin PaulinoNo ratings yet
- Global Warming in The PhilippinesDocument1 pageGlobal Warming in The PhilippinesAldrin PaulinoNo ratings yet
- Sample FDAR (Nursing)Document1 pageSample FDAR (Nursing)Aldrin PaulinoNo ratings yet
- A. Narrative Evaluation of Actual Nursing ProblemsDocument1 pageA. Narrative Evaluation of Actual Nursing ProblemsAldrin PaulinoNo ratings yet
- A. Narrative Evaluation of Actual Nursing ProblemsDocument1 pageA. Narrative Evaluation of Actual Nursing ProblemsAldrin PaulinoNo ratings yet
- The Influence of The English Language On The Russian Youth SlangDocument10 pagesThe Influence of The English Language On The Russian Youth SlangВасилий БоровцовNo ratings yet
- Arabic in UrduDocument5 pagesArabic in UrduNanang Nurcholis0% (1)
- Office Furniture Catalogue EnquiryDocument12 pagesOffice Furniture Catalogue EnquiryAdela MărgineanuNo ratings yet
- Daniel Bell's Concept of Post-Industrial Society: Theory, Myth, and IdeologyDocument42 pagesDaniel Bell's Concept of Post-Industrial Society: Theory, Myth, and IdeologyTeni ChitananaNo ratings yet
- Set Down Servant!: . J J J. ' F R - 'Document7 pagesSet Down Servant!: . J J J. ' F R - 'Kora LapaNo ratings yet
- Environmental Impact Assessment (EIA) in Nepal: Ministry of Population and EnvironmentDocument11 pagesEnvironmental Impact Assessment (EIA) in Nepal: Ministry of Population and EnvironmentAden ShahuNo ratings yet
- Prisoner of ZendaDocument27 pagesPrisoner of ZendaSauban AhmedNo ratings yet
- Financial Performance and Position HighlightsDocument100 pagesFinancial Performance and Position HighlightsSHAMSUL ARIF ZULFIKAR HUSNINo ratings yet
- Reminder Letter For Requisie Documents For MonitoringDocument1 pageReminder Letter For Requisie Documents For MonitoringFarah RoyNo ratings yet
- TNB Electricity System Voltages, Frequencies, Earthing Systems and Supply OptionsDocument4 pagesTNB Electricity System Voltages, Frequencies, Earthing Systems and Supply OptionsSaiful RizamNo ratings yet
- CII IF2-General Insurance Business-1Document276 pagesCII IF2-General Insurance Business-1paschalpaul722100% (1)
- DuniaDocument64 pagesDuniaAmith PanickerNo ratings yet
- Answers To Gospel QuestionsDocument4 pagesAnswers To Gospel QuestionsCarlos Andrés ValverdeNo ratings yet
- IndiaMart Research ProjectDocument15 pagesIndiaMart Research ProjectbusinessideasNo ratings yet
- Bharat MalaDocument29 pagesBharat MalaNavin GoyalNo ratings yet
- Pigovian Welfare Economics 3Document4 pagesPigovian Welfare Economics 3vikram inamdar100% (1)
- CLJ5 - Evidence Module 3: Rule 129: What Need Not Be Proved Topic: What Need Not Be ProvedDocument9 pagesCLJ5 - Evidence Module 3: Rule 129: What Need Not Be Proved Topic: What Need Not Be ProvedSmith BlakeNo ratings yet
- Engineering Department: Northern RailwayDocument113 pagesEngineering Department: Northern RailwayKrisna SinghNo ratings yet
- National DanceDocument2 pagesNational DanceJohn Paul CasaclangNo ratings yet
- Petition for issuance of second owner's duplicate titleDocument2 pagesPetition for issuance of second owner's duplicate titlebernard jonathan Gatchalian100% (1)
- Black Violet Pink 3D Company Internal Deck Business PresentationDocument16 pagesBlack Violet Pink 3D Company Internal Deck Business Presentationakumar09944No ratings yet
- Perceptual Thinking StyleDocument5 pagesPerceptual Thinking StyleAmirul Faris50% (2)
- PaperDocument4 pagesPaperAnne ChenNo ratings yet
- Lesson 4 Jobs and Occupations PDFDocument2 pagesLesson 4 Jobs and Occupations PDFronaldoNo ratings yet
- Jim McElwain ContractDocument15 pagesJim McElwain ContractColoradoanNo ratings yet
- Letter Sa Mga Panel Inag FinalsDocument7 pagesLetter Sa Mga Panel Inag FinalsCHENNY BETAIZARNo ratings yet
- UntitledDocument22 pagesUntitledArjun kumar ShresthaNo ratings yet
- IMI ScriptDocument130 pagesIMI ScriptDiego JacobsNo ratings yet