You might also like
- Perception and CoordinationDocument7 pagesPerception and CoordinationSonia G. Ortiz0% (1)
- Pcip-Ncmh 2016Document38 pagesPcip-Ncmh 2016Carissa De Luzuriaga-BalariaNo ratings yet
- Health Assessment Powerpoint (Assessing Newborn and Infant)Document33 pagesHealth Assessment Powerpoint (Assessing Newborn and Infant)rick_wb0% (1)
- Administering Enema POWERPOINT GIVING ENEMA TO PATIENT, FOR PATIENT WITH GASTROINTESTINAL DISORDERS .. LECTURES, PRINCIPLES AND PROCEDURESDocument14 pagesAdministering Enema POWERPOINT GIVING ENEMA TO PATIENT, FOR PATIENT WITH GASTROINTESTINAL DISORDERS .. LECTURES, PRINCIPLES AND PROCEDURESPb0% (1)
- Cultural CompetenceDocument70 pagesCultural Competencekatejewel de rosasNo ratings yet
- Nursing Informatics FrameworkDocument3 pagesNursing Informatics FrameworkEstelle RhineNo ratings yet
- Historical MethodDocument33 pagesHistorical MethodSharmaine BeranNo ratings yet
- Assessing The Nose and SinusesDocument5 pagesAssessing The Nose and SinusesYudi TrigunaNo ratings yet
- Filipino Culture, Values and Practices in Relation To Health Care of Individual and FamilyDocument15 pagesFilipino Culture, Values and Practices in Relation To Health Care of Individual and Familyfatima dasalNo ratings yet
- IV Return DemoDocument2 pagesIV Return Demognikap_deleonNo ratings yet
- Vital SignsDocument2 pagesVital SignsstaciadokNo ratings yet
- Impact of Pandemic To The Psychological Aspects of Nursing StudentsDocument25 pagesImpact of Pandemic To The Psychological Aspects of Nursing StudentsBrandon AreteNo ratings yet
- CTP 102-ADocument7 pagesCTP 102-AJose Marco Dela CruzNo ratings yet
- Elec 121Document14 pagesElec 121MARITONI MEDALLANo ratings yet
- Administering An EnemaDocument2 pagesAdministering An EnemaJazzmin Angel ComalingNo ratings yet
- COPAR: Community Participatory Action ResearchDocument5 pagesCOPAR: Community Participatory Action ResearchEdezer CariasNo ratings yet
- Focus Charting in Pediatric Ward: Medsurgical ClinicalDocument2 pagesFocus Charting in Pediatric Ward: Medsurgical Clinical2A - Nicole Marrie HonradoNo ratings yet
- Unit 2 Topic 4 STSDocument6 pagesUnit 2 Topic 4 STSRachell AvecillaNo ratings yet
- Geria Lec Portfolio CasiaDocument9 pagesGeria Lec Portfolio CasiaMarie Ashley CasiaNo ratings yet
- Nursing Care of A Family With A Toddler Child: Christine M. Fiel, RN MN LPT MaedDocument25 pagesNursing Care of A Family With A Toddler Child: Christine M. Fiel, RN MN LPT MaedJrose CuerpoNo ratings yet
- ETHICAL AND LEGAL ASPECTS OF HEALTH EDUCATIONDocument4 pagesETHICAL AND LEGAL ASPECTS OF HEALTH EDUCATIONMaria Angelika BughaoNo ratings yet
- A Case Study On Pediatric Community Acquired Pneumonia-DDocument58 pagesA Case Study On Pediatric Community Acquired Pneumonia-DAnonymous A5dkn4N3No ratings yet
- Updated Revised-Open Gloving Technique ChecklistDocument6 pagesUpdated Revised-Open Gloving Technique ChecklistRalf FiedalinoNo ratings yet
- Chapter 056Document19 pagesChapter 056Michael SamaniegoNo ratings yet
- P.A. 1Document6 pagesP.A. 1SamSarah BongolanNo ratings yet
- HA-RLE-WS # 3 Assessing Mental Status and Substance AbuseDocument7 pagesHA-RLE-WS # 3 Assessing Mental Status and Substance AbuseJULIE ANNE CORTEZNo ratings yet
- Personal Hygiene: Mary Grace L. Araullo RN MSCPDDocument23 pagesPersonal Hygiene: Mary Grace L. Araullo RN MSCPDgraceNo ratings yet
- Skill Performance Evaluation - Measuring Intake and OutputDocument2 pagesSkill Performance Evaluation - Measuring Intake and OutputLemuel Que100% (1)
- A. B. C. D. E. F. G.: Crutch-WalkingDocument4 pagesA. B. C. D. E. F. G.: Crutch-WalkingGene BulaNo ratings yet
- Assessing the Thorax and LungsDocument26 pagesAssessing the Thorax and LungsTarah LedesmaNo ratings yet
- Theoretical FrameworkDocument2 pagesTheoretical FrameworkLisette CastilloNo ratings yet
- Admitting Patient: When Admitting A Patient What Are The Basic Procedures?Document4 pagesAdmitting Patient: When Admitting A Patient What Are The Basic Procedures?diah ayuNo ratings yet
- Per Cutaneous Trans Hepatic Cholangiogram (PTC)Document15 pagesPer Cutaneous Trans Hepatic Cholangiogram (PTC)Hamzeh AlmasriNo ratings yet
- Pedia Nursing Lecture on Growth and DevelopmentDocument59 pagesPedia Nursing Lecture on Growth and Developmentshenric16100% (1)
- Campinha Bacote2002 PDFDocument4 pagesCampinha Bacote2002 PDFJudy Anne PatricioNo ratings yet
- Capillary Blood Glucose (CBG) Examination Study Guide: NCM - 116 - Related Learning Experience (Skills and ClinicalDocument15 pagesCapillary Blood Glucose (CBG) Examination Study Guide: NCM - 116 - Related Learning Experience (Skills and ClinicalAlma Janella TOSINONo ratings yet
- Case Scenario - NebulizationDocument2 pagesCase Scenario - NebulizationHilario. Hayascent.Reign.M.No ratings yet
- 5 Three Mental OperationsDocument12 pages5 Three Mental OperationsSherwin Pazzibugan100% (1)
- 04 Singular, Particular, Universal Terms.Document26 pages04 Singular, Particular, Universal Terms.jailene padreNo ratings yet
- Prelim Exam NCM 103Document10 pagesPrelim Exam NCM 103Zhyraine Iraj D. CaluzaNo ratings yet
- Code of Ethics For Registered NursesDocument7 pagesCode of Ethics For Registered NursespampamaosNo ratings yet
- Perioperative Risks & InterventionsDocument5 pagesPerioperative Risks & InterventionsJellou MacNo ratings yet
- Feeding Via Gastric GavageDocument3 pagesFeeding Via Gastric Gavageneleh gray0% (1)
- Assessing The NeckDocument3 pagesAssessing The NeckAnne Joyce Lara AlbiosNo ratings yet
- Gordons Functional Health Patterns GuideDocument4 pagesGordons Functional Health Patterns GuideteuuuuNo ratings yet
- CATHETERIZATION ChecklistDocument2 pagesCATHETERIZATION Checklistjmmos207064No ratings yet
- Topic 1 Concepts in The Care of At-Risk & Sick Adult ClientsDocument1 pageTopic 1 Concepts in The Care of At-Risk & Sick Adult ClientsChristine Joy MolinaNo ratings yet
- PRC Form (Minor Operation)Document1 pagePRC Form (Minor Operation)mawelNo ratings yet
- Community Health Assessment ToolsDocument54 pagesCommunity Health Assessment ToolsDANICA FRANCONo ratings yet
- Cues Nursing Diagnosis Background and Knowledge Goals and Objectives Nursing Intervention and Rationale EvaluationDocument3 pagesCues Nursing Diagnosis Background and Knowledge Goals and Objectives Nursing Intervention and Rationale EvaluationKristiene Kyle AquinoNo ratings yet
- UNIT 6 The Nursing Role in Supporting The Health of Ill Children and Their FamiliesDocument5 pagesUNIT 6 The Nursing Role in Supporting The Health of Ill Children and Their FamiliesStephanie LeeNo ratings yet
- Newborn Care ProceduresDocument5 pagesNewborn Care Proceduresallkhusairy6tuansiNo ratings yet
- NGT LavageDocument2 pagesNGT LavageAngela Joy AmparadoNo ratings yet
- ) Administering Nasogastric Tube or Orogastric Tube FeedingDocument6 pages) Administering Nasogastric Tube or Orogastric Tube FeedingJohn Pearl FernandezNo ratings yet
- Nursing Case Analysis FeliDocument20 pagesNursing Case Analysis FeliIanusGwapitusNo ratings yet
- BS Nursing Program OutcomesDocument20 pagesBS Nursing Program Outcomesۦۦ JamesNo ratings yet
- Healthcare Reflections, Insights, and Lessons: Proactive/ReactiveFrom EverandHealthcare Reflections, Insights, and Lessons: Proactive/ReactiveNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Nursing History and Gordon'sDocument2 pagesNursing History and Gordon'sCarlo bersamiraNo ratings yet
- NURSING HEALTH HISTORY FOR OLDER PERSON Version01Document4 pagesNURSING HEALTH HISTORY FOR OLDER PERSON Version01MICAELA QUINAJONNo ratings yet
- NAVORA MidtermDocument2 pagesNAVORA MidtermNavora, Bryle TrixthaneNo ratings yet
- Laguna Copperplate InscriptionDocument4 pagesLaguna Copperplate InscriptionNavora, Bryle TrixthaneNo ratings yet
- Universidad de Manila: Republic of The Philippines City of ManilaDocument2 pagesUniversidad de Manila: Republic of The Philippines City of ManilaNavora, Bryle TrixthaneNo ratings yet
- Navra Case StudyDocument4 pagesNavra Case StudyNavora, Bryle TrixthaneNo ratings yet
- Bienvenido Tantco Sr.Document2 pagesBienvenido Tantco Sr.Navora, Bryle TrixthaneNo ratings yet
- FINAL Module 1A Health Education PerspectiveDocument12 pagesFINAL Module 1A Health Education PerspectiveNavora, Bryle TrixthaneNo ratings yet
- Defining CommunicationDocument3 pagesDefining CommunicationNavora, Bryle TrixthaneNo ratings yet
- Art Appreciation - Activity 1Document1 pageArt Appreciation - Activity 1Navora, Bryle TrixthaneNo ratings yet
- Template For Functional Health Pattern AssessmentDocument2 pagesTemplate For Functional Health Pattern AssessmentNavora, Bryle TrixthaneNo ratings yet
- Isolation of crude catalase extract from potatoDocument3 pagesIsolation of crude catalase extract from potatoNavora, Bryle TrixthaneNo ratings yet
- Conducting Health Interview or Nursing Health History: I. Biographical DataDocument5 pagesConducting Health Interview or Nursing Health History: I. Biographical DataNavora, Bryle TrixthaneNo ratings yet
- Approach To Basic Nursing SkillsDocument9 pagesApproach To Basic Nursing SkillsNavora, Bryle TrixthaneNo ratings yet
- EXP #7 Iodine TestDocument2 pagesEXP #7 Iodine TestNavora, Bryle TrixthaneNo ratings yet
- Instructions: Explain Comprehensively The Following Questions. To Be Submitted in Google Drive. With The File Name (SURNAME, FIRST NAME)Document2 pagesInstructions: Explain Comprehensively The Following Questions. To Be Submitted in Google Drive. With The File Name (SURNAME, FIRST NAME)Navora, Bryle TrixthaneNo ratings yet
- Universidad de Manila: Department of NursingDocument4 pagesUniversidad de Manila: Department of NursingNavora, Bryle TrixthaneNo ratings yet
- Experiment #3 Title: Millon's Test: Performed On: Performed byDocument3 pagesExperiment #3 Title: Millon's Test: Performed On: Performed byNavora, Bryle TrixthaneNo ratings yet
- Output #2Document1 pageOutput #2Navora, Bryle TrixthaneNo ratings yet
- Cell Surface Tension ExperimentDocument3 pagesCell Surface Tension ExperimentNavora, Bryle TrixthaneNo ratings yet
- Experiment #6 Title: Barfoed's Test: Performed On: Performed byDocument3 pagesExperiment #6 Title: Barfoed's Test: Performed On: Performed byNavora, Bryle TrixthaneNo ratings yet
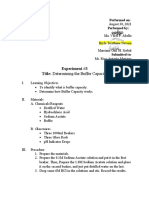
- EXP #2 Determining Buffer CapacityDocument3 pagesEXP #2 Determining Buffer CapacityNavora, Bryle TrixthaneNo ratings yet
- EXP #8 Bromination of Unsaturated Fatty AcidsDocument3 pagesEXP #8 Bromination of Unsaturated Fatty AcidsNavora, Bryle TrixthaneNo ratings yet
- NSTP Activity ReportDocument2 pagesNSTP Activity ReportNavora, Bryle TrixthaneNo ratings yet
- EXP #3 Denaturation of Proteins Through CoagulationDocument3 pagesEXP #3 Denaturation of Proteins Through CoagulationNavora, Bryle TrixthaneNo ratings yet
- Cell Surface Tension ExperimentDocument3 pagesCell Surface Tension ExperimentNavora, Bryle TrixthaneNo ratings yet
- College of Health Sciences: Course Syllabus Course InformationDocument19 pagesCollege of Health Sciences: Course Syllabus Course InformationNavora, Bryle Trixthane100% (1)
- Reflective Learning SheetDocument1 pageReflective Learning SheetNavora, Bryle TrixthaneNo ratings yet
- Millon's Test for Protein DetectionDocument3 pagesMillon's Test for Protein DetectionNavora, Bryle TrixthaneNo ratings yet
- All Answers Must Be Elaborated and Well Explained: Navora, Bryle Trixthane D. 09/29/2021Document2 pagesAll Answers Must Be Elaborated and Well Explained: Navora, Bryle Trixthane D. 09/29/2021Navora, Bryle TrixthaneNo ratings yet
- NSTP ReportDocument4 pagesNSTP ReportNavora, Bryle TrixthaneNo ratings yet
- International Journal of Obstetric AnesthesiaDocument6 pagesInternational Journal of Obstetric Anesthesiaanita pratiwiNo ratings yet
- Illinois Eye Exam Report RequirementsDocument2 pagesIllinois Eye Exam Report RequirementsRichard BakerNo ratings yet
- Understanding Perceptual Sensitivity and Decision CriteriaDocument3 pagesUnderstanding Perceptual Sensitivity and Decision CriteriaHarshit ShrivastavaNo ratings yet
- MATERIAL SAFETY DATA SHEET 3M™ Novec ™ 1230 Fire Protection Fluid (FK-5-1-12)Document8 pagesMATERIAL SAFETY DATA SHEET 3M™ Novec ™ 1230 Fire Protection Fluid (FK-5-1-12)Juan LuisNo ratings yet
- Post Tonsillectomy Bleeding Clinical Practice GuidelineDocument5 pagesPost Tonsillectomy Bleeding Clinical Practice Guidelinemohamed fahmyNo ratings yet
- Ashgate - Landscape Professional Practice PDFDocument281 pagesAshgate - Landscape Professional Practice PDFyondaimethunderNo ratings yet
- Catarina Grilo Enfermage M: Escola Superior de Saúde Ribeiro SanchesDocument478 pagesCatarina Grilo Enfermage M: Escola Superior de Saúde Ribeiro SanchesDaniela Pisa100% (1)
- Veterinary EctoparasitesDocument8 pagesVeterinary Ectoparasitesc3891446100% (1)
- Effectiveness of Mesotherapy On Body Contouring: BackgroundDocument7 pagesEffectiveness of Mesotherapy On Body Contouring: BackgroundNita Dewi NNo ratings yet
- Catch Up Fridays Blank Week 2Document5 pagesCatch Up Fridays Blank Week 2jessyl cruzNo ratings yet
- Planeacion Preoperatoria Artroplastia CaderaDocument8 pagesPlaneacion Preoperatoria Artroplastia Caderamontserrat santiago sanchezNo ratings yet
- E.Coli Essay FINAL PDFDocument8 pagesE.Coli Essay FINAL PDFSaraturituriNo ratings yet
- Pianakafinal Sa Lahatt RyannDocument14 pagesPianakafinal Sa Lahatt RyannPaul IglesiasNo ratings yet
- Muscle Strength TestingDocument3 pagesMuscle Strength TestingGiselle Chloe Baluya ico100% (1)
- Personal Protective Equipment - GustinaDocument24 pagesPersonal Protective Equipment - GustinaHidayatullah HidayatullahNo ratings yet
- The Influence of Transactional Leadership of Police Commissioned Officers and Quality of Work Life On Organizational Commitment Among Police Non-Commissioned OfficersDocument9 pagesThe Influence of Transactional Leadership of Police Commissioned Officers and Quality of Work Life On Organizational Commitment Among Police Non-Commissioned OfficersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Healthy Eating Habits GuidelineDocument30 pagesHealthy Eating Habits GuidelineSuhanidah MyNo ratings yet
- IBPS Prelims CallDocument5 pagesIBPS Prelims CallPrakash RajNo ratings yet
- Denah Mixed Use LT 3 &4Document1 pageDenah Mixed Use LT 3 &4Jennifer MadenNo ratings yet
- LanoLip Power Point PresentationDocument12 pagesLanoLip Power Point PresentationWalter Sanchez EscobarNo ratings yet
- Project Report On Health & Safety PDFDocument3 pagesProject Report On Health & Safety PDFAakash SolankiNo ratings yet
- OET 3 Reading Test 17 Part ADocument5 pagesOET 3 Reading Test 17 Part AAlice ChirilaNo ratings yet
- Igcse Biology Concepts Revision Chapter 1 To 8Document9 pagesIgcse Biology Concepts Revision Chapter 1 To 8naduniNo ratings yet
- OJT PORTFOLIO REDCROSS4A - RoveliDocument52 pagesOJT PORTFOLIO REDCROSS4A - RoveliRaffy Liwan Kalinga ChapterNo ratings yet
- 4.health 8 Law Q2 21 22 PDFDocument8 pages4.health 8 Law Q2 21 22 PDFwensleyarcillaNo ratings yet
- Safety Data Sheet: Section 1. IdentificationDocument9 pagesSafety Data Sheet: Section 1. IdentificationJivendra KumarNo ratings yet
- Cognitive Interventions in Mature and Older Adults, Benefits For Psychological Well-Being and Quality of LifeDocument12 pagesCognitive Interventions in Mature and Older Adults, Benefits For Psychological Well-Being and Quality of LifeGabrielle PradoNo ratings yet
- Resona r9 Platinum Multi Parametric Breast SolutionDocument2 pagesResona r9 Platinum Multi Parametric Breast SolutionXing LuNo ratings yet
- Verification of Medical Condition(s) : Instructions For The Customer Information For The DoctorDocument3 pagesVerification of Medical Condition(s) : Instructions For The Customer Information For The DoctorElise SloperNo ratings yet
- Benefits of Intermittent FastingDocument3 pagesBenefits of Intermittent FastingSaurabh PandeyNo ratings yet